“Government U-Turn on Prescription Co-Payment Fees: A Critical Analysis of Policy Incompetence” - 11 January 2026

The New Zealand government’s handling of prescription co-payment fees for 12-month prescriptions reveals a troubling pattern of policy incompetence, poor planning, and inadequate consideration of patient welfare. The reversal of the original decision to charge patients $5 every three months exposes significant flaws in the government’s decision-making processes and healthcare policy implementation.
The Policy Reversal: What Happened
In May 2025, as part of Budget 2025, the government initially decided that patients would need to pay a $5 co-payment fee every three months when collecting medicines under the new 12-month prescription policy. This decision was made specifically “to mitigate the financial impact on Health New Zealand,” as revealed by RNZ. However, Cabinet documents released just before Christmas revealed that this decision was rescinded in September 2025, with patients now only paying the fee once at the first collection.
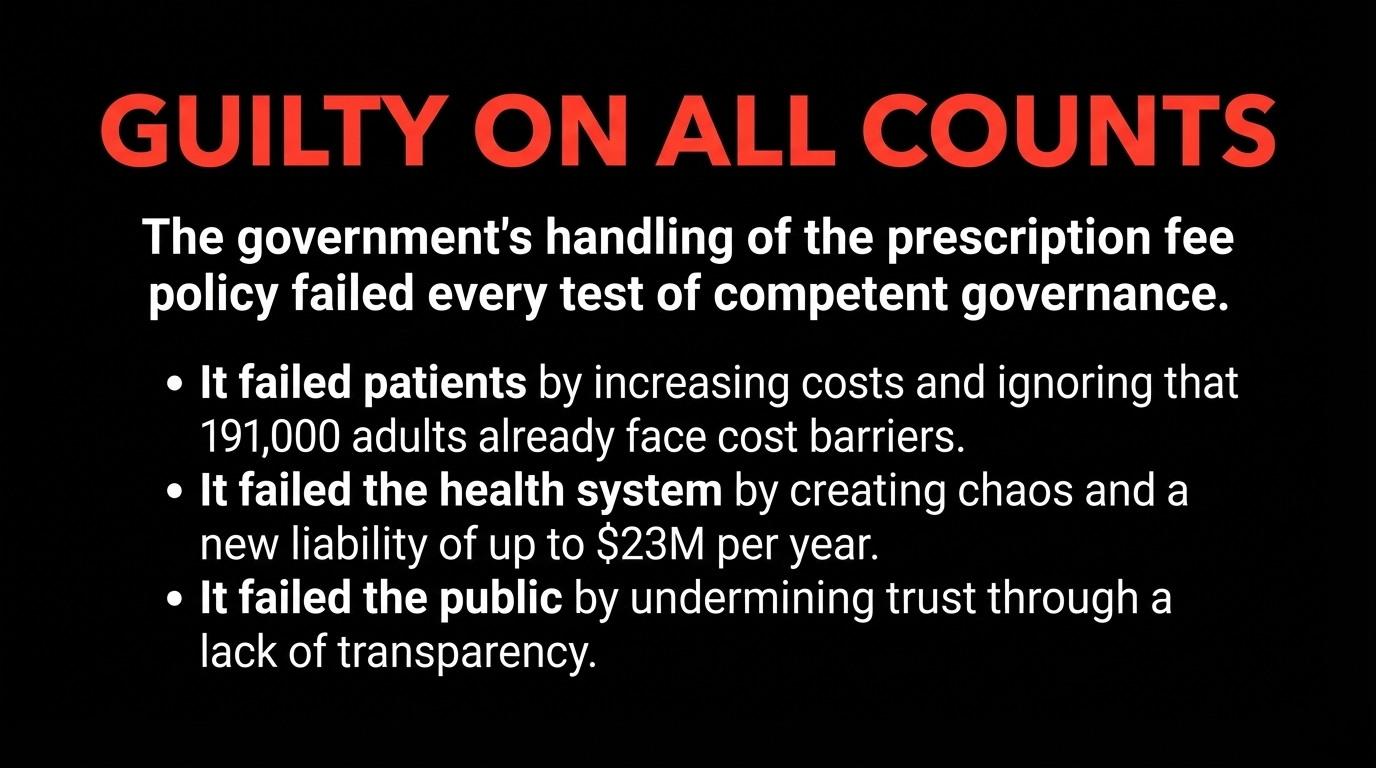
Health Minister Simeon Brown admitted in Cabinet papers that “the previous decision does not align with the policy intent to reduce costs to patients,” according to RNZ’s reporting. This statement is damning—it reveals the government made a decision in May that fundamentally contradicted its own stated policy objectives. The reversal means patients will save up to $15 annually, but it will cost Health NZ between $6 million and $23 million per year, with costs estimated to grow by approximately 5% annually, as reported by the NZ Herald.
Fundamental Policy Incompetence
Contradicting Stated Objectives
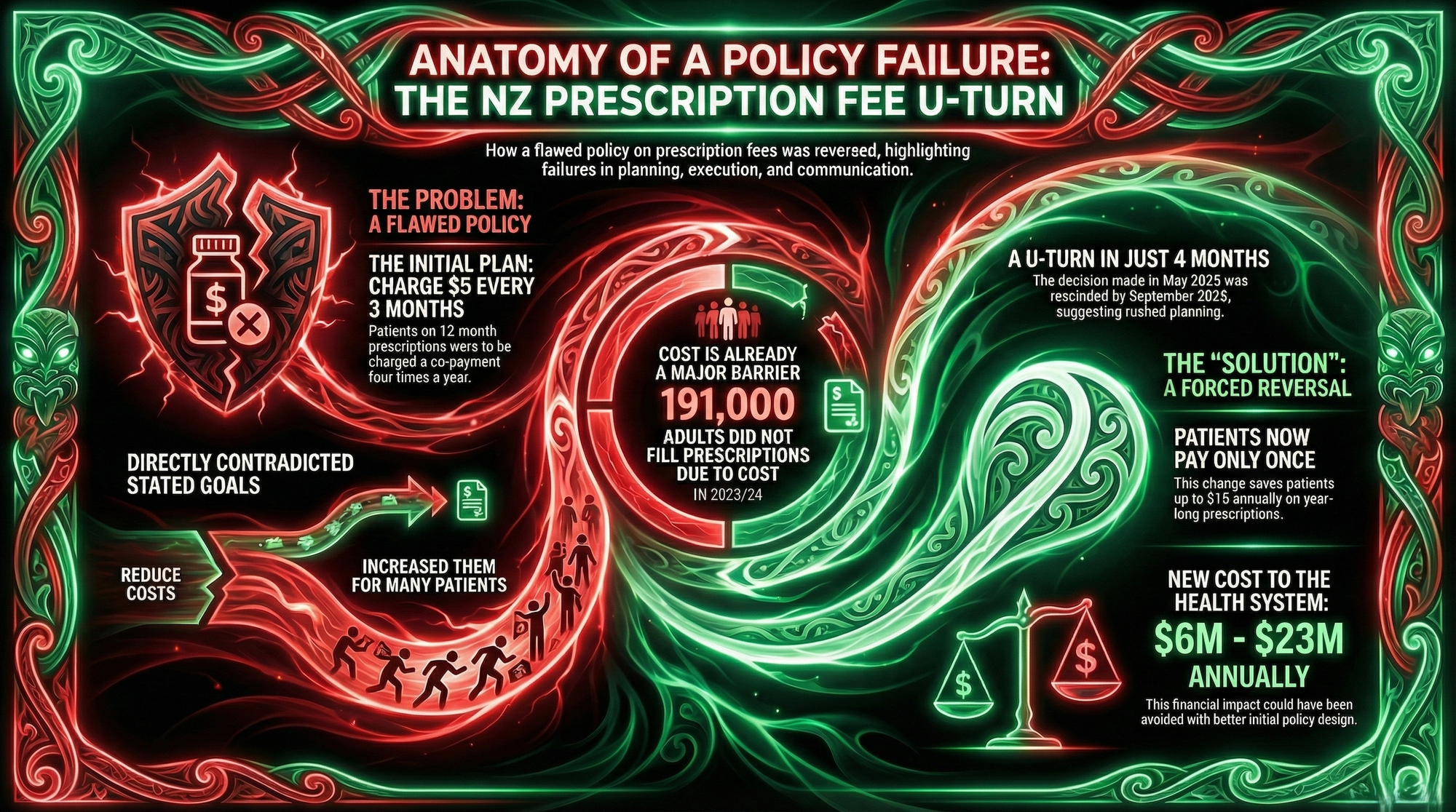
The government announced 12-month prescriptions as a way “to reduce the cost of seeing GPs” and remove “unnecessary barriers for patients,” as stated in RNZ’s coverage. Yet the initial decision to charge patients $5 every three months for a year-long prescription directly undermined this goal. This represents a fundamental failure of policy coherence—designing a cost-saving measure that would actually increase costs for patients with chronic conditions who need regular medication pickups.
Research shows that approximately 191,000 adults in 2023/24 did not fill prescriptions due to cost barriers, according to RNZ. Studies have demonstrated that eliminating prescription co-payments has substantial effects on reducing hospitalizations. One analysis found that people unable to afford prescriptions were approximately 30% more likely to be admitted to hospital compared to control groups, costing New Zealand’s healthcare system in excess of $2.65 billion annually, as discussed on Reddit. Against this evidence, the decision to multiply prescription fees was staggeringly shortsighted.
Rushed Decision-Making Without Adequate Analysis
The initial decision to charge fees every three months was made in May ahead of Budget 2025, yet by September—just four months later—the government had to reverse course. This timeline suggests inadequate consultation with stakeholders, insufficient analysis of patient impacts, and failure to properly model the policy’s effects before announcement. The fact that Cabinet papers acknowledged the decision would “reduce complexity for Health NZ” and address “financial implications for both Health NZ and Pharmac” indicates these considerations should have been obvious from the outset.
Communication Failures and Lack of Transparency
The reversal was buried in documents released three days before Christmas—a time traditionally used for releasing politically sensitive information when public attention is low. While the government did include bullet points about the single co-payment in media materials sent to reporters in November, these were absent from the public version on the Beehive website and conflicted with earlier reports without clearly explaining the policy change, as noted by RNZ.
This lack of transparency is particularly problematic given that Pharmac Review findings specifically highlighted concerns about “the transparency and accessibility of decision-making processes” in New Zealand’s health system. The government’s handling of this reversal demonstrates continued failures in transparent communication with the public about health policy changes that directly affect their finances and access to care.
Broader Context of Health System Failures
Systemic Problems at Health NZ
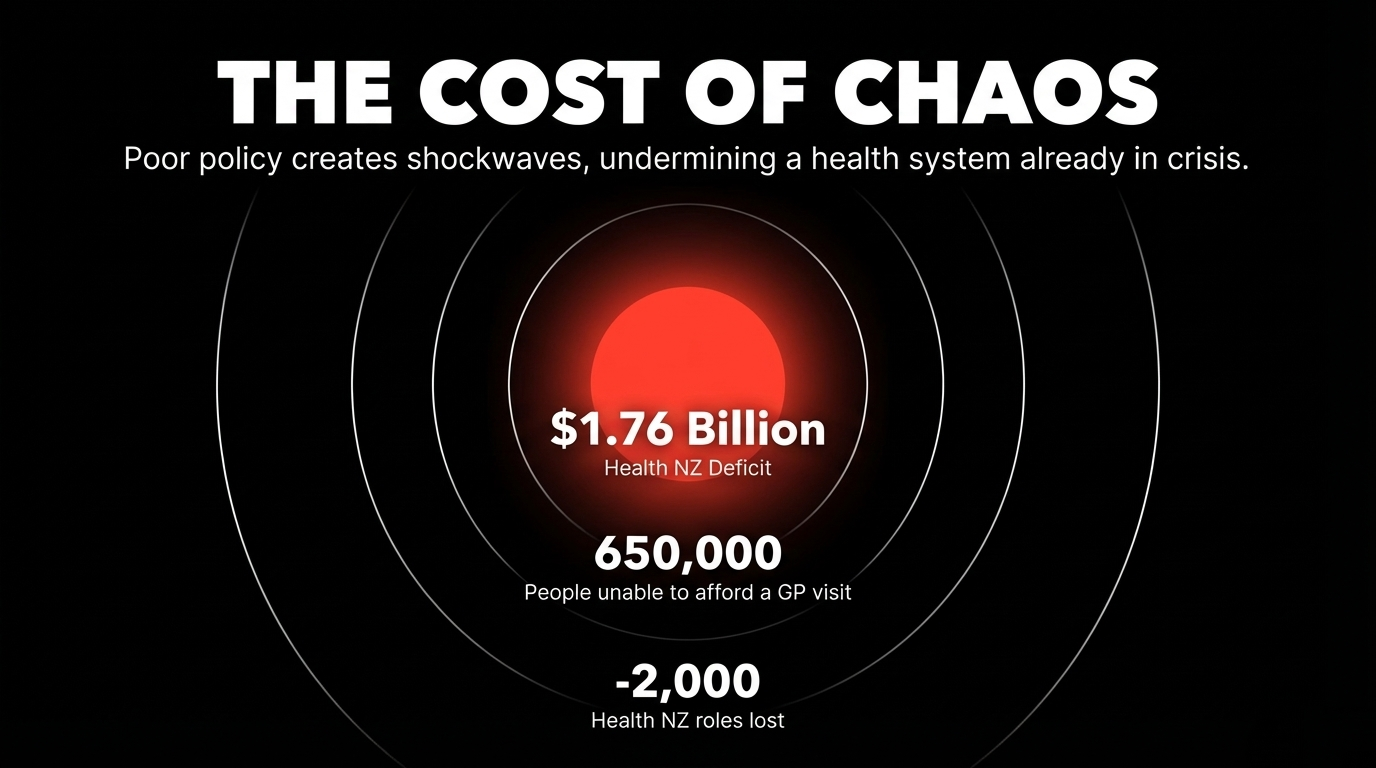
This prescription fee debacle is not an isolated incident but part of a broader pattern of governance failures in New Zealand’s health system under this government. The Health NZ deficit ballooned to $1.76 billion, with the organization struggling with financial planning and cohesion.
Continuing Access Barriers
Despite claims of improving healthcare access, Labour’s analysis revealed that nearly 650,000 people cannot afford to see their family doctor—an increase of over 100,000 since the current government took office. One in four Pacific adults cannot afford doctor visits, and 87,000 people avoid doctors because they already owe money to their clinic, an increase of 11,000 in one year.
The reinstatement of the $5 prescription co-payment in July 2024 (after Labour had abolished it), as reported by 1News, already represented a barrier to access. The initial plan to charge this fee quarterly for 12-month prescriptions would have compounded this barrier.
Budget Shortfalls and Cuts
Analysis by the Association of Salaried Medical Specialists found that the 2025/26 health budget falls short by nearly $250 million to cover inflation, demographic changes, and new initiatives. Meanwhile, hospitals were asked to save $510 million despite $538 million going unspent last year due to unfilled vacancies.
This financial context makes the prescription co-payment flip-flopping particularly egregious. The government was willing to save $6-23 million annually at the expense of patient access and administrative complexity, only to reverse the decision months later after criticism—demonstrating reactive rather than proactive, evidence-based policymaking.
Healthcare Professional and Pharmacy Sector Concerns
Clinical and Safety Implications
Healthcare professionals have raised serious concerns about the 12-month prescription policy itself, beyond just the payment structure. Dr. Angus Chambers warned that leaving patients for 12 months without review could lead to “more emergency department visits and hospital admissions,” as reported by the Economic Times. Professor Rinki Murphy highlighted risks of “missed side effects or complications” and reduced opportunities for medication reviews.
These clinical concerns were apparently not adequately addressed during the policy development phase. The fact that the co-payment structure had to be reversed suggests similar rushed planning characterized the entire 12-month prescription initiative.
Pharmacy Sector Impact
Prior to the Labour government’s removal of prescription fees, pharmacists were estimated to spend 2-3 hours per day on administrative work related to collecting fees, sorting payment plans, and chasing outstanding bills rather than practicing pharmacology, as noted on Reddit.
Pharmacy Guild chief executive Andrew Gaudin welcomed the u-turn, noting it ensures “more affordable access for patients to medicines, GPs, and community pharmacies,” according to RNZ. The fact that the pharmacy sector relief is notable underscores how the original quarterly charging decision would have created significant administrative burden and complexity—impacts that should have been obvious during policy development.
Pattern of Policy U-Turns and Failures
Repeated Course Reversals
This prescription co-payment reversal is part of a troubling pattern of policy u-turns by the Coalition government. Other examples include:
- Winston Peters’ open criticism of the Regulatory Standards Bill after the government promoted it, as reported by 1News
- Failures to deliver promised cancer drug funding as originally announced, with the Health Minister later admitting the policy “should have been communicated better” and implementation challenges weren’t adequately considered, according to the NZ Herald
Lack of Evidence-Based Decision-Making
Despite coalition agreements promising evidence-based decisions, changes have frequently “favoured corporate interests and wealthy donors at the expense of ordinary citizens, often in defiance of expert advice,” as noted by the Integrity Institute. The prescription policy reversal exemplifies this pattern—the initial decision prioritized Health NZ’s immediate financial position over patient welfare and the substantial evidence showing prescription charges reduce medication adherence and increase downstream health costs.
Workforce and Capacity Implications
Staff Reductions Undermining Capacity
The Public Health Agency faces job cuts to emergency management and pandemic preparedness, with the biggest impacts in emergency management (from 11 roles to 2) and Māori Public Health (from 6 staff to 2). The Public Service Association warned these cuts leave New Zealand “vulnerable” as disease and disaster risks increase. Professor Michael Baker noted that “with every one of these re-organisations and downsizing processes, we’re losing expertise and momentum.”
These capacity reductions make coherent policy development increasingly difficult. Fewer expert staff means less thorough policy analysis, weaker implementation planning, and greater likelihood of errors like the prescription co-payment fiasco.
Delayed OIA Responses and Accountability
Health Minister Brown blamed officials for slow Official Information Act responses, yet the Public Service Association correctly noted that “he can’t keep demanding savings and then blame officials when the impacts of cuts are felt.” Health NZ has lost over 2,000 roles, including teams supporting information requests. Labour’s Carmel Sepuloni warned that New Zealand’s reputation for transparency “has been compromised by this government.”
This reduced transparency and accountability makes it harder for the public and stakeholders to scrutinize policy decisions before implementation—contributing to errors like the prescription charging reversal.
A Case Study in Incompetence
The prescription co-payment u-turn represents a case study in policy incompetence. The government:
- Made an initial decision that contradicted its own stated policy objectives
- Failed to adequately analyze patient impacts, administrative burden, and evidence about prescription cost barriers
- Rushed the decision without proper consultation
- Had to reverse course just four months later
- Released the reversal in a manner designed to minimize scrutiny
- Imposed costs on Health NZ ($6-23 million annually) that could have been avoided with proper initial planning
This failure occurred within a broader context of health system dysfunction, workforce cuts, budget shortfalls, worsening access indicators, and repeated policy reversals. Rather than demonstrating competent, evidence-based governance, the episode reveals reactive decision-making, inadequate planning, and policy development processes that prioritize short-term fiscal considerations over patient welfare and long-term health system sustainability.
For a government that claims to be “focused on reducing costs and making it simpler and more convenient for patients to access the medicines they need,” as stated in the Beehive announcement, this prescription policy debacle demonstrates precisely the opposite: increased complexity, confused messaging, wasted time and resources, and a decision-making process that put patients last until forced to backtrack by criticism. The incompetence is not merely in making one wrong decision, but in the systematic failures of planning, analysis, consultation, and implementation that allowed such an obviously flawed policy to proceed in the first place.

Ivor Jones The Māori Green Lantern Fighting Misinformation and Disinformation From The Far Right