“The House That Colonialism Built: Quantifying the Cost of Breaking Our Foundation” - 29 January 2026

Mōrena Aotearoa,
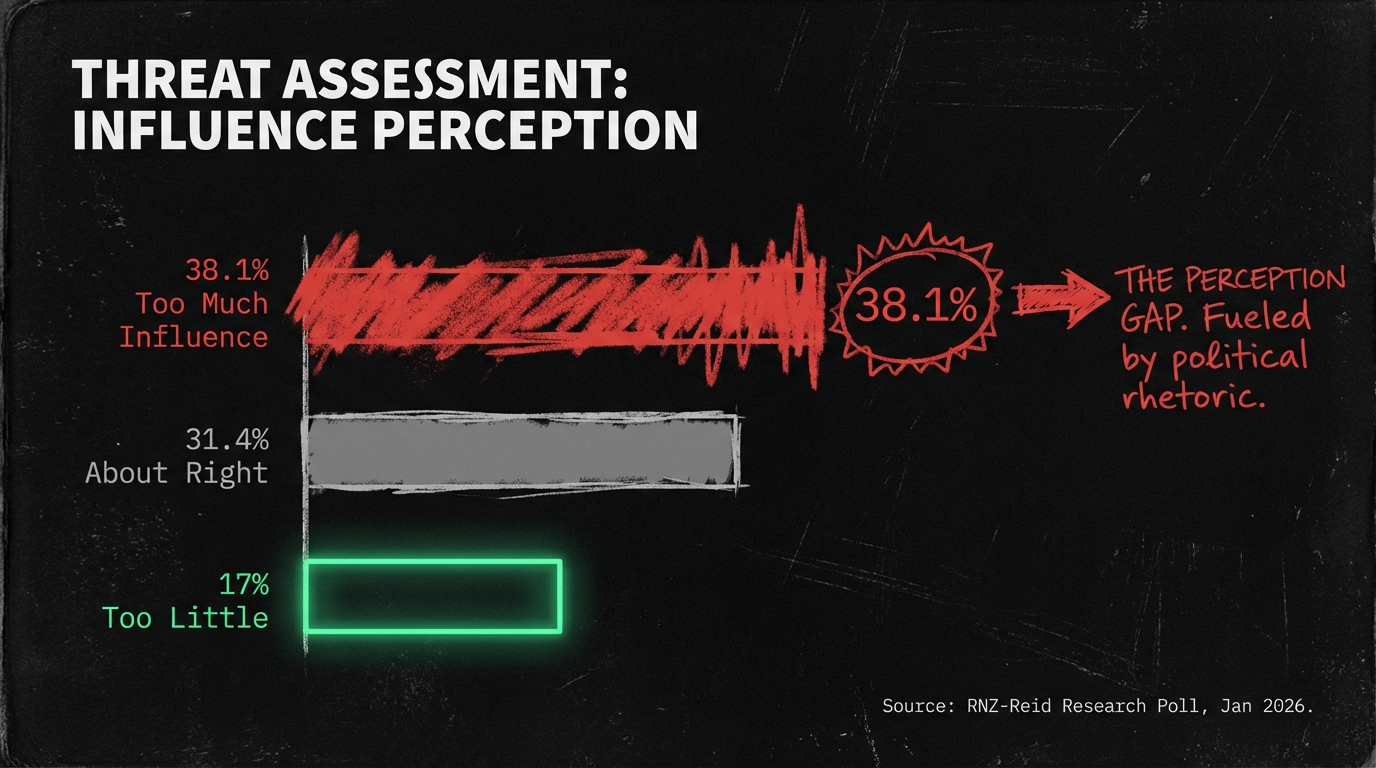
In January 2026, a poll revealed that 38.1 percent of New Zealanders believe Te Tiriti o Waitangi has “too much” influence on government decisions.
This perception exists in stark contrast to quantifiable reality:
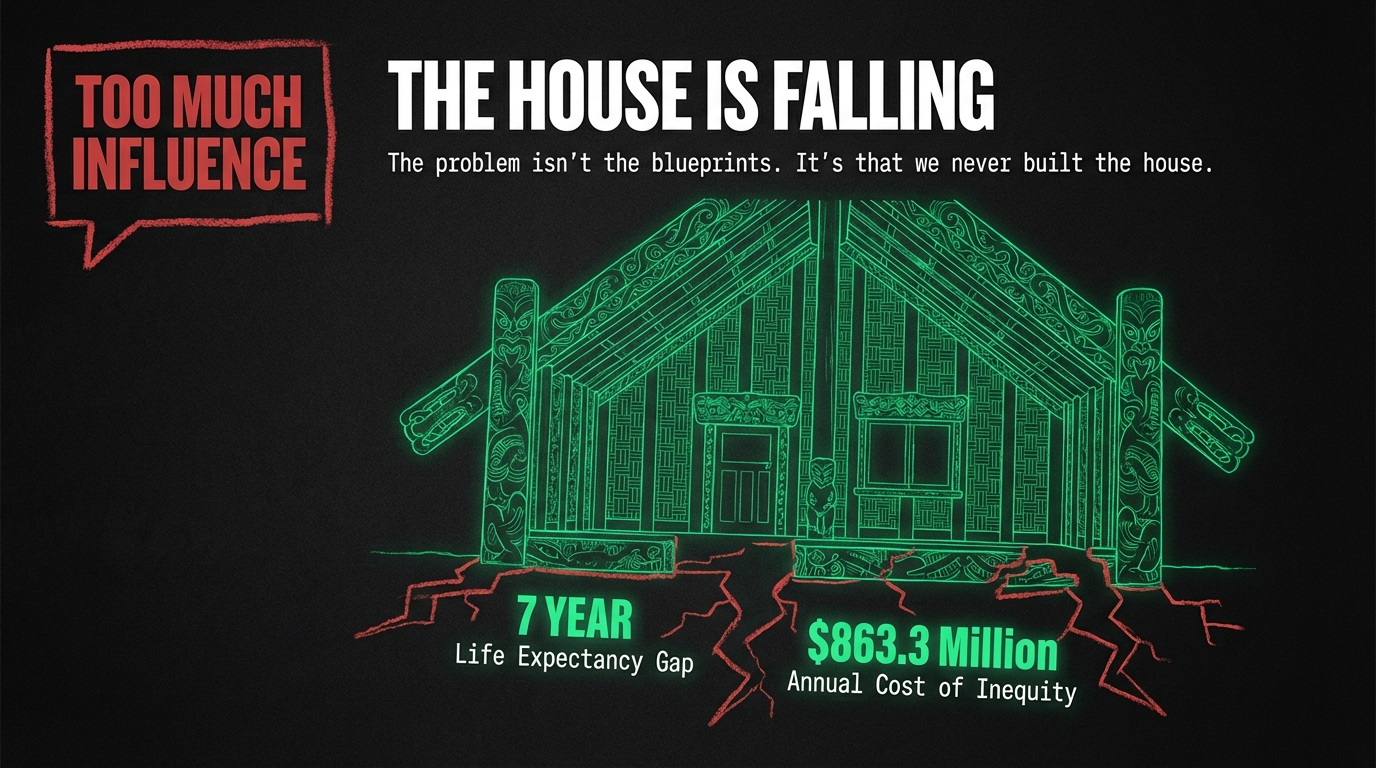
the Crown’s failure to honor Treaty obligations costs New Zealand $863.3 million annually in Māori health inequities alone,
with Māori living seven years less than non-Māori and
the health system actively profiting from underservicing Indigenous communities by $75.7 million per year.
When a house is falling, occupants often blame the architect’s blueprints rather than acknowledging the deterioration. The Treaty is not the problem. The problem is that we have never built the house it promised.
The Architecture of Inequality: Foundations Built on Sand
The Promise and the Reality
In 1840, two nations signed architectural plans for a shared dwelling—a compact that guaranteed Māori would retain tino rangatiratanga (sovereignty) over their lands, villages, and taonga (treasures) while allowing the Crown to govern. Article Three extended British subject rights to Māori, promising equal citizenship while respecting distinct authority.
The English and Māori texts diverged significantly, with 500 signatories signing the Māori version versus only 39 signing the English.
As former Chief Justice Sian Elias stated,
“it can’t be disputed that the Treaty is actually the Māori text.”
Yet from the foundation-laying, the Crown began constructing a different house entirely. Through systematically dismantling the original design, successive governments have created structural defects that now manifest as quantifiable, measurable harm.
The Crumbling Framework: Health Inequities as Structural Failure
Consider health outcomes as the house’s foundation. When foundations crack, the entire structure becomes uninhabitable. The Waitangi Tribunal’s WAI 2575 inquiry found the Crown breached Te Tiriti by failing to design and administer the primary health system to address Māori health inequities. This is not rhetorical failure—it is measurable structural collapse:
Life Expectancy Gap: The Foundation’s Depth
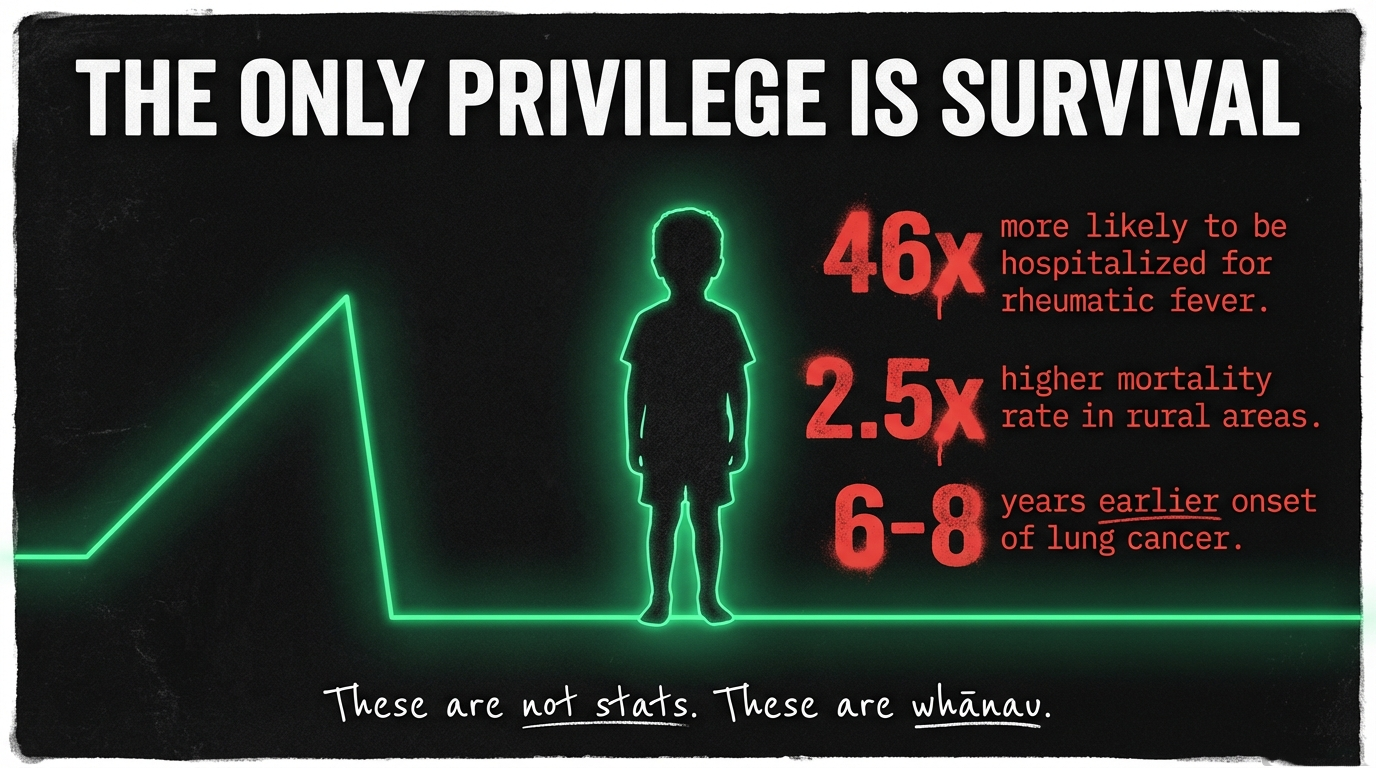
Māori women die 7 years earlier than European/Other women, while Māori men die 8 years earlier than their European counterparts. The gap persists at 6.4 years for men and 5.5 years for women in the most recent data. Over half of Māori deaths are attributed to avoidable causes—deaths that would not occur if the Crown had fulfilled its Treaty obligations.
Disease Burden: The Load-Bearing Walls
Māori develop lung cancer 6-8 years earlier than non-Māori at lower smoking exposure. Ischaemic heart disease rates are 2× higher for Māori adults, while Māori females have lung cancer registration rates 3× higher than non-Māori females. Perhaps most devastating: Māori children are 46× more likely to be hospitalized with acute rheumatic fever versus European children, while Pasifika children face 115× higher hospitalization rates for the same preventable disease.
Rural Mortality: The Remote Wings
In rural communities, the structural failure intensifies. Rural Māori experience all-cause mortality rates 2.22-2.54× higher than non-Māori. In the most remote communities, age-standardized mortality is 2.5× higher for Māori, with Māori 1.8× as likely to die from preventable causes compared to non-Māori in large cities.
Mental Health and Discrimination: The Interior Climate
18.2% of Māori report high psychological distress, while 13.8% of Māori experienced racial discrimination in the past year (2020/21), up from 10.8% in 2011/12. For Māori women, discrimination rose from 9.7% to 16.8% over the same period. Racial discrimination is directly associated with higher psychological distress, lower self-rated health, and higher unmet healthcare needs, with twenty-four quantitative studies confirming the link between discrimination and poorer health outcomes.
These are not abstract statistics. They represent 7,245 excess Māori deaths between 2003 and 2014—lives that would not have been lost if Māori experienced the same amenable mortality rate as non-Māori.
Profiting from Decay: The Economic Architecture of Underservicing
The Perverse Financial Incentives

Perhaps most revealing is that the Crown financially benefits from failing Māori. The health system does not bear the cost of inequity—it profits from it.
The Balance Sheet of Institutional Racism
The total annual cost of Māori adult health inequities:
$863.3 million. Of this, direct health system costs account for only $39.9 million (excess hospitalizations, outpatient care), while indirect costs of $823.4 million are borne by Māori families and society through years of life lost and lost wages.
Meanwhile, primary care saves $49.4 million per year by underserving Māori, while accident/injury care saves $26.3 million per year through Māori underutilization. Less than 5% of the cost is borne by the health system itself. The vast majority—$823.4 million annually—is borne directly by Māori whānau and communities through premature death and lost economic productivity.
As health equity researchers concluded, “The net impact for the government health sector is that it saves millions per year in underservicing Māori, even when excess hospitalisations are taken into account”. Another expert termed this “an unconscionable breach of human rights and a dereliction of duty by the New Zealand health system”.
The Business Case Against Equity
Professor Rhema Vaithianathan identified the structural problem succinctly:
Under capitation funding models where District Health Boards owned hospitals but never owned privately-operated primary care,
“the business case for primary care to reduce inequity in the health system is simply not there”.
This represents a system designed to externalize costs onto those least able to bear them while concentrating profits among private providers. It is economic architecture that would never pass basic ethical review.
The Waitangi Tribunal’s Verdict: A House Built on Treaty Breaches
Crown Breaches Documented
The Waitangi Tribunal found the Crown breached Treaty obligations by:
- Failing to design and administer the primary health system to address Māori health inequities
- Underfunding Māori primary health organizations from the outset
- Remaining aware of failures for well over a decade yet failing to amend policies
- Not collecting enough qualitative/quantitative data to understand sector performance for Māori
- Te Puni Kōkiri’s failure of its statutory duty to monitor health sector effectiveness for Māori
Funding Inequities Exposed
Over $200 billion was spent on health since 2012, with little measurable improvement to Māori outcomes. Of this staggering sum, only $167 million (less than 0.1%) was allocated for primary care of Māori patients, and only $28.7 million went to Māori primary health organizations during this period.
Accountability Failures
Perhaps most damning: the Crown has never withheld money, never sacked a DHB board, never rejected an annual plan due to poor Māori health performance. The system contains no consequences for failure.
The Treaty Principles Bill: Demolishing What Little Remains
While 38.1% of voters believe the Treaty has “too much” influence, the Treaty Principles Bill was overwhelmingly opposed in submissions to Parliament. The Select committee process was estimated to cost ~$6 million, and the Select committee ultimately recommended the Bill not proceed. All parties except ACT voted against it (11 for, 112 against).
Harms Identified
Health experts warned the Bill would:
- Undermine Māori sovereignty, rights, and protections
- Facilitate corporate exploitation and environmental harm
- Entrench an “institutionally racist” health system
- Exacerbate health disparities and increase racist rhetoric against Māori
- Reverse progress toward treaty justice
The Regulatory Standards Bill, described as “as serious and dangerous as” the Treaty Principles Bill, could “wipe hundreds of millions of dollars off historic settlement values”. The Waitangi Tribunal recommended an “immediate halt” to the Bill.
The Opportunity Cost: What We Sacrifice by Breaking Treaty Obligations
Treaty Settlements: The Two Cents on the Dollar
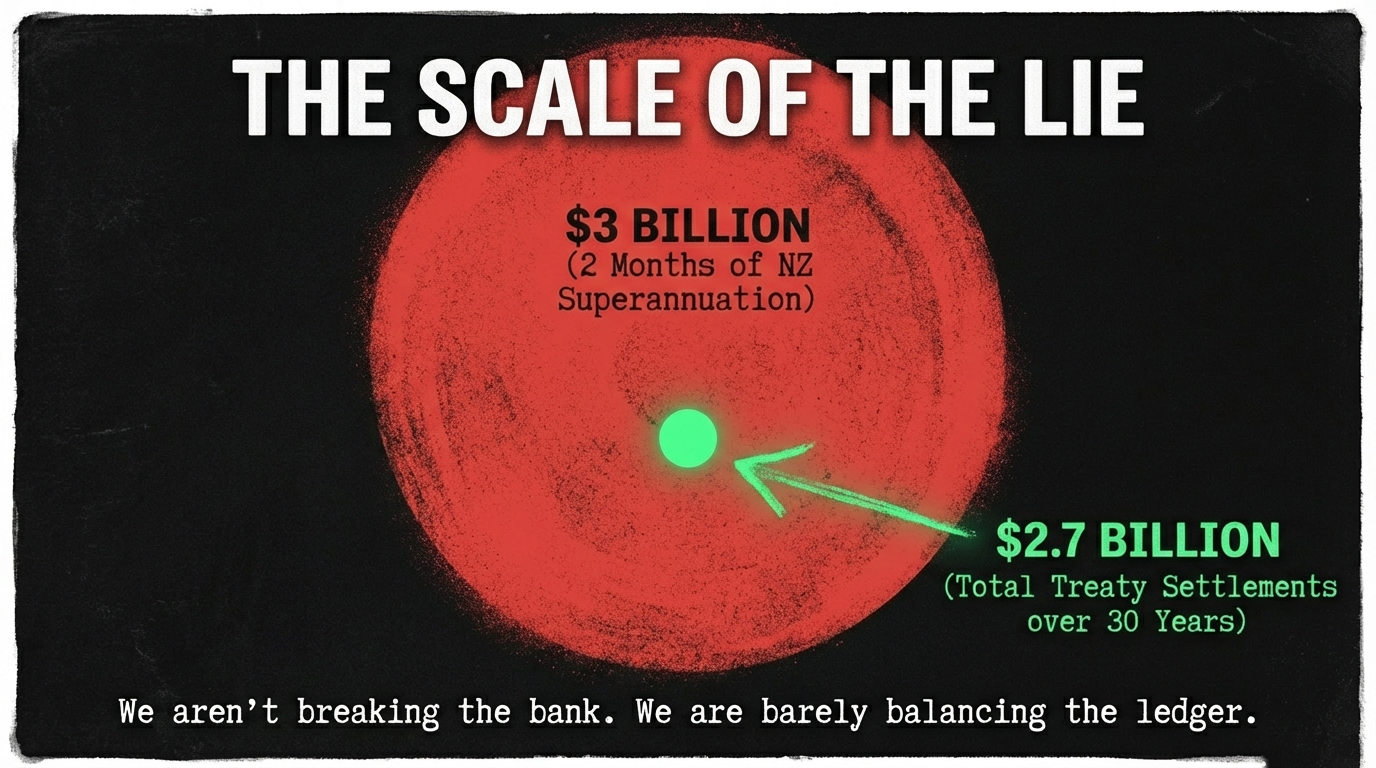
The Crown has negotiated 88 settlements totaling approximately $2.73-2.738 billion in financial and commercial redress. To contextualize: the government spends $19 billion on superannuation annually—total Treaty settlements represent less than two months of superannuation spending. Or consider: the government bailed out South Canterbury Finance investors to the tune of $1.775 billion in 2010—nearly as much as 30 years of Treaty redress.
Yet these modest settlements have generated extraordinary economic returns. Ngāi Tahu received $170 million in 1998 and grew its asset base to over $2 billion within 25 years—a tenfold increase. Waikato-Tainui’s $170 million settlement (1995) grew to $2.4 billion in assets by 2025.
The Thriving Māori Economy
The Māori economy contribution to GDP grew from $17 billion (6.5%) in 2018 to $32 billion (8.9%) in 2023. The Māori asset base increased 83%—from $69 billion to $126 billion—over this period. The ten largest post-settlement iwi now hold $8.2 billion in assets, with iwi-owned commercial entities outperforming many of New Zealand’s largest listed companies on a return-on-assets basis.
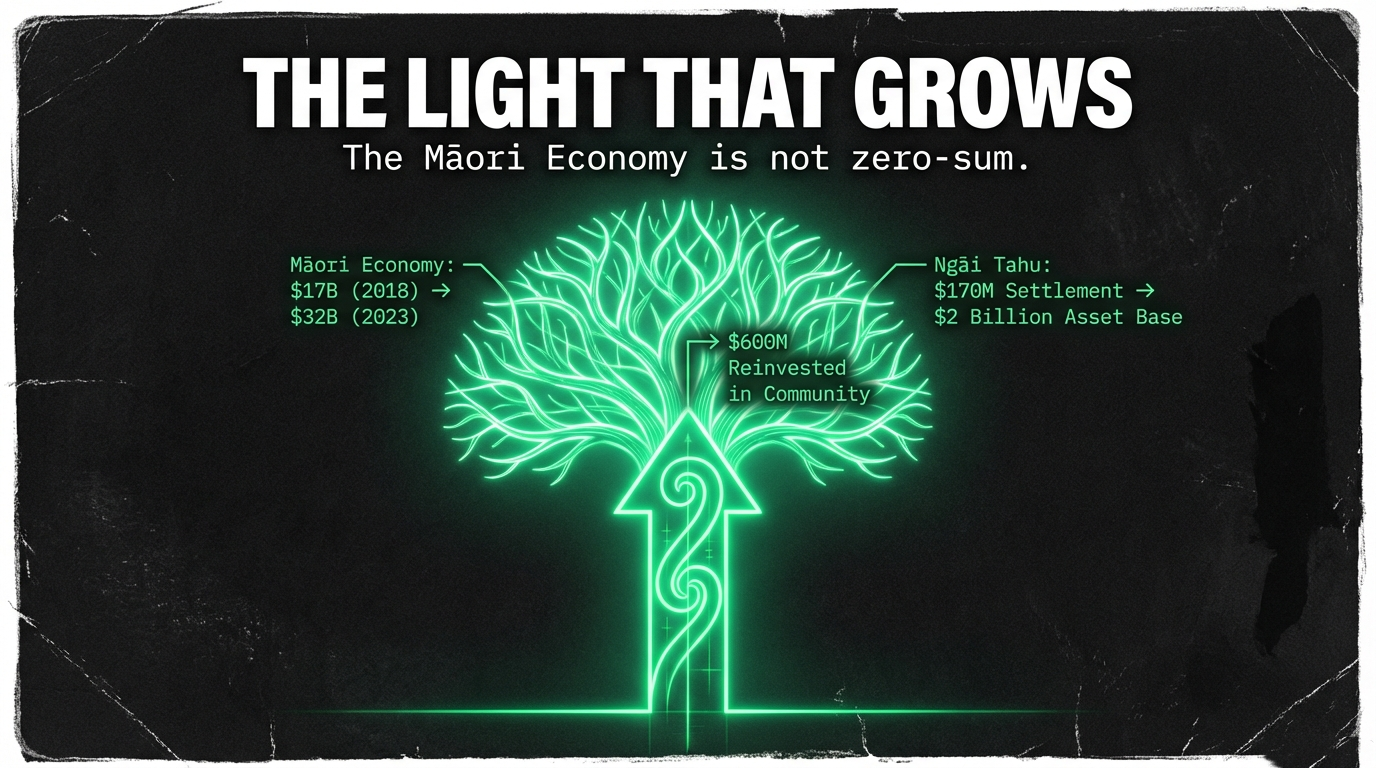
Ngāi Tahu has distributed $600 million into tribal development since settlement, investing in housing, education, and cultural revitalization including te reo Māori. In 2025, Waikato-Tainui entered a $1 billion joint venture with global investment firm Brookfield—described as “the single largest investment that this tribe has undertaken” in 30 years.
This is not zero-sum economics. When the Māori economy grows, all New Zealanders benefit through job creation, infrastructure development, and economic diversification. Iwi businesses prioritize reinvestment in communities, job creation, and long-term sustainability over short-term profit extraction.
What Works: Evidence-Based Solutions
The perception that the Treaty has “too much” influence obscures a more pressing reality: we have barely begun implementing what works. The evidence is clear:
Māori-Led Health Providers Deliver Results
Māori health providers delivered 33,330 vaccinations by June 2024, surpassing the Government’s goal of 10,000 set in March 2024—more than tripling the target. During the COVID-19 pandemic, Māori providers faced bureaucratic hurdles and were initially sidelined by officials, yet when finally resourced, achieved massive increases in vaccination rates—as much as 20% in towns like Kawerau and Te Teko in a single month.
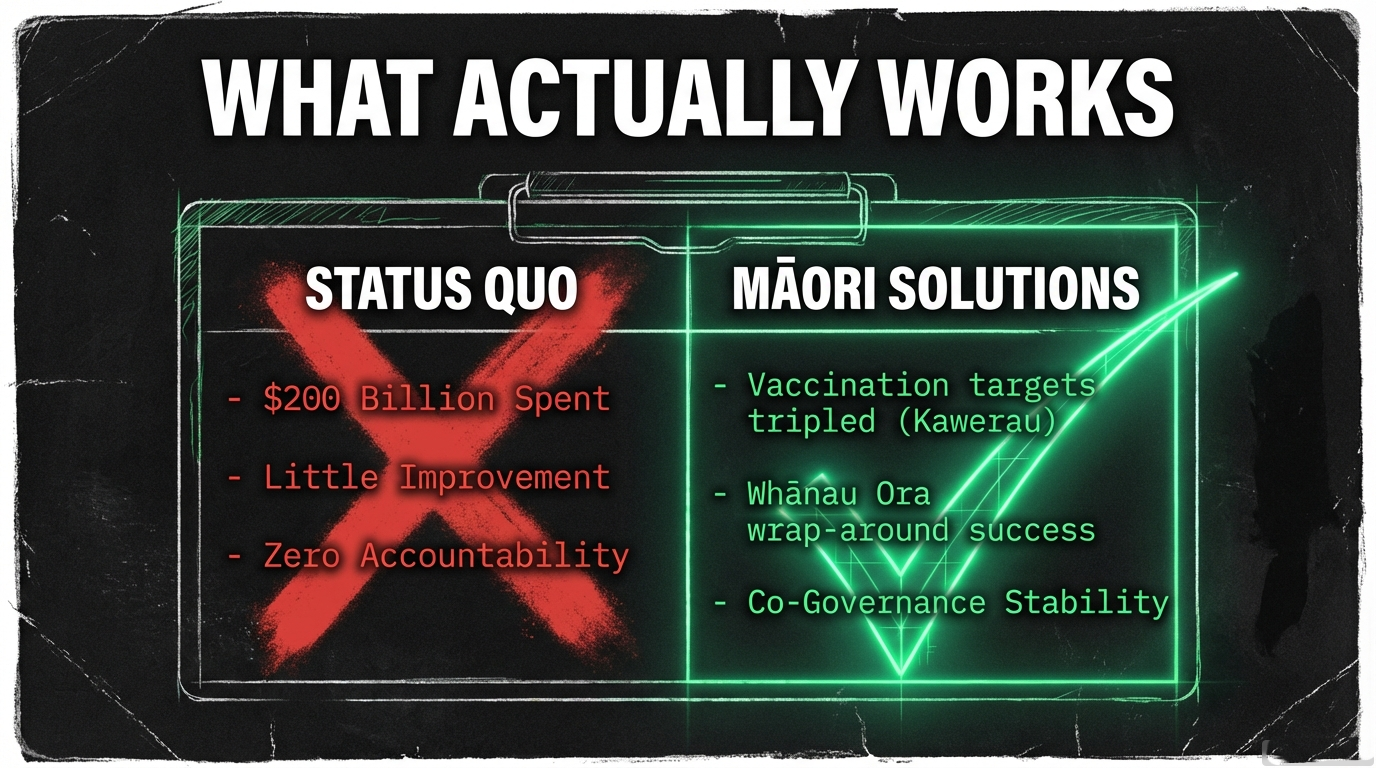
Whānau Ora, established in 2010, provides wrap-around health and social services in a whānau context, demonstrating the effectiveness of culturally-grounded, holistic approaches. Ngāti Porou Hauora, an East Coast Māori health provider, became a Primary Health Organisation with community-embedded kaiawhina (health navigators) who possess intimate knowledge of people and their needs—a model that has delivered measurably better outcomes.
Co-Governance Works
Despite political controversy, co-governance arrangements have “worked very well” according to former Treaty Negotiations Minister Chris Finlayson, who negotiated numerous settlements.
The Waikato River Authority, created in 2010, operates as a single board with shared Crown-iwi representation.
Its chief executive noted they do not have a
—the board operates with a clear shared purpose.
As Deputy Chair Ngarimu Blair stated:
Iwi Māori Partnership Boards (IMPBs), established in 2022, represent over 900,000 Māori and were created to address inequities within the health system.
Former MP Louisa Wall noted the boards focus on primary intervention
—”engaging earlier and not at the hospital”
—precisely where the system is most inefficient.
“We’re just starting to get traction and make a real difference”,
she said, before the current government moved to diminish their statutory role.
Structural Solutions Required
- Eliminate financial barriers to primary care: 22% of Māori experience cost barriers to GP visits (vs 13% non-Māori), while 14% face cost barriers to prescriptions (vs 5% non-Māori). The Treasury estimates the economic cost of ill-health at $10-27 billion per year—making GP and dental care free would cost $3+ billion but save vastly more in avoided hospitalizations.
- Reform primary care funding: The current model saves $49.4 million/year by underserving Māori with no financial incentive to rectify inequities. Higher capitation for high-needs populations (Māori, Pacific, deprived areas) would align incentives with outcomes.
- Strengthen Treaty accountability: The Crown has never withheld funding or sacked a DHB board for poor Māori health performance. Mandatory health equity analysis in all economic decisions and performance data stratified by ethnicity would create genuine accountability.
- Restore/strengthen Māori health authority: Te Aka Whai Ora was disestablished after just 18 months. The Waitangi Tribunal found disestablishment breached Treaty obligations. WAI 2575 concluded the primary health system has failed Māori; Māori solutions are needed.
Building the House We Were Promised
The poll finding that 38.1% of voters believe the Treaty has “too much” influence reveals a profound disconnect between perception and reality.
The Treaty doesn’t have too much influence
—it has too little.
What we call “Treaty influence” is actually the minimum scaffolding preventing total structural collapse.
The metaphor is precise:
we live in a house built on broken promises. The original architectural plans guaranteed partnership, protection, and participation. Instead, we constructed a dwelling that enriches itself by shortening Māori lives by seven years, that profits $75.7 million annually from underservicing Indigenous communities, that costs the economy $863.3 million in preventable health inequities.
And when Māori point to the cracks in the foundation
—when the Waitangi Tribunal documents Crown breaches,
when health researchers quantify the $200 billion spent with “little measurable improvement” to Māori outcomes,
when 7,245 excess deaths accumulate
—we are told the problem is the Treaty having “too much influence.”
The evidence tells a different story. When Treaty obligations are honored—when Māori providers receive adequate resources, when co-governance arrangements allow iwi expertise to guide decision-making, when $170 million settlements grow to $2 billion and create economic opportunity for entire regions—everyone benefits.
The Crown has already paid tens of millions in compensation for failing to meet settlement commitments. The government is managing 12,000 contractual/legal commitments across 150 public organizations, with system-wide monitoring “not where it should be”.
The risk isn’t that the Treaty has too much influence. The risk is that we continue building on a broken foundation, that compensation costs outstrip settlement values, that we sacrifice $863 million annually because fixing the system would require acknowledging we never built what we promised.
The house is falling not because the blueprints were wrong, but because we never followed them. The question isn’t whether the Treaty has too much influence. The question is whether we have the courage to finally build the house it promised—a dwelling strong enough for all of us to call home.
Koha Consideration: Funding the Foundations We Were Promised
Every koha for this kaupapa is a decision to stop living in a house built on cracks and start funding the rebuild ourselves. It is a refusal to accept a system that profits from Māori dying seven years earlier, that banks $75 million a year from underservicing our people, and then tells us the Treaty has “too much” influence.
Koha is not charity. It is rangatiratanga in action—the power to fund our own truth-tellers when Crown and corporate structures will not. It is how we pay for the measuring tools, the torches, and the blueprints that expose where the foundations have failed and what it will take to repair them.
If this essay helped you see the real cost of broken Treaty promises—if it sharpened your arguments, resourced your organising, or simply made you angrier in a more informed way—consider a koha to keep this work going.
Kia kaha, whānau. Stay vigilant. Stay connected. And if you are able, choose one of these pathways to support this mahi:
- Koha platform (direct support for this mahi)
Koha—Support: https://app.koha.kiwi/events/the-maori-green-lantern-fighting-misinformation-and-disinformation-ivor-jones - Substack subscription (receive essays + support the work)
Subscribe to the Māori Green Lantern on Substack: https://themaorigreenlantern.substack.com/subscribe - Direct bank transfer (for those who prefer straight to the pūtea)
Account name: HTDM
Account number: 03-1546-0415173-000
Every contribution—small or large—helps fund the accountability that the current system will never voluntarily deliver. It keeps the lights on in this whare of evidence, analysis, and unapologetic truth.

Ivor Jones The Māori Green Lantern Fighting Misinformation And Disinformation From The Far Right