“THE PRESCRIPTION FOR PRIVATISATION” - 24 October 2025
How the Herald and Government Collude to Starve Public Healthcare While Māori Die Waiting
Kia ora e te whānau. Tēnā koutou katoa.
Paywalled article: https://www.dropbox.com/scl/fi/kyzsrvv6ncebtg00dniu5/Fish-hooks-and-cautious-support_-GPs-weigh-up-Labour-s-new-health-policy-NZ-Herald.PDF?rlkey=r7pkelfyzgmwmlfd3c96mkyeq&st=ozujhnfz&dl=0
Here is the brutal truth that Derek Cheng and the New Zealand Herald do not want you to understand:
Underfunded Māori healthcare, killed thousands of our people through delayed care, and prepared the ground for full privatisation of primary care - https://www.nzherald.co.nz/nz/politics/fish-hooks-and-cautious-support-gps-weigh-up-labours-new-health-policy/FVMSDWUOQJGTTOMXQOWER5LXQA/.
This article from NZME - a corporatised media conglomerate now under pressure from billionaire shareholder Jim Grenon who demands “editorial balance” and has openly attacked trans rights, Treaty obligations, and progressive journalism - masquerades as neutral analysis while concealing the fundamental colonial violence embedded in New Zealand’s health system.
The real story is not about Labour’s tepid policy proposal or the Coalition’s modest funding increase. The real story is about how the Waitangi Tribunal’s WAI 2575 inquiry proved beyond doubt that the Crown has breached Te Tiriti o Waitangi by systematically underfunding Māori primary healthcare providers by at least $531 million since 2003, causing an estimated $5 billion in annual health loss in 2018 alone. The real story is how both Labour and National governments have weaponised austerity against Māori bodies while quietly redirecting public healthcare toward private profit.
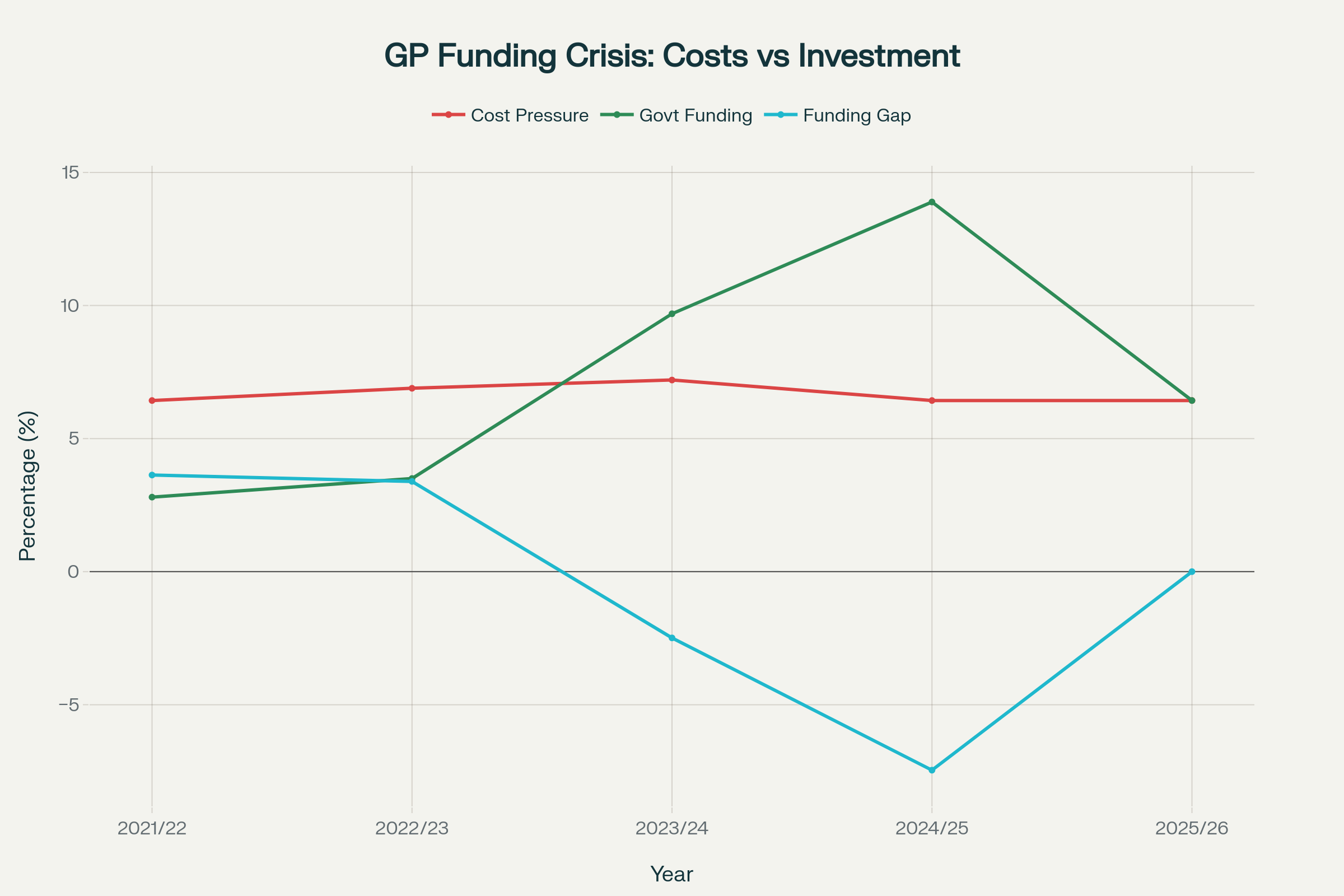
Government funding for GPs has consistently fallen short of actual cost pressures, creating a structural funding crisis that forces practices to either raise patient fees or close their books to new enrollments
Background
To understand this manufactured crisis, you must first understand how primary care funding actually works - and how it has been deliberately designed to fail Māori. Since 2002, GP clinics receive capitation funding based on the number of enrolled patients, with rates determined primarily by age and gender using data from the late 1990s. This antiquated formula completely ignores ethnicity, multimorbidity, socioeconomic deprivation, and the actual health needs of high-needs populations.
The Waitangi Tribunal found this funding mechanism is fundamentally inequitable and embeds historical inequity by systematically underfunding services for Māori. When the actual costs of running a GP practice increase by 6.43 percent annually, but government funding in 2025/26 only increases by 6.43 percent after years of massive shortfalls - with no catchup for decades of underfunding - practices have only two choices: massively increase patient fees or close their books to new patients.
The Coalition Government claims it provided $175 million in additional funding, a 13.89 percent increase. Health Minister Simeon Brown - a fundamentalist Christian conservative with a documented history of anti-abortion activism, opposition to LGBTQI+ rights, and membership in a church that actively placed members into National Party positions - has declared this “record investment” proves underfunding claims are “fake news”. Yet independent analysis shows GP practices need between $353 million and $1.36 billion to address unmet need, and the 2022 Sapere report found very high-need practices would require funding increases between 34 percent and 231 percent to deliver appropriate care.
Meanwhile, the current capitation formula systematically underfunds Māori providers who serve predominantly Māori populations with significantly higher health needs. These providers serve patients with multiple chronic conditions, living in high deprivation areas, facing structural barriers to care - yet receive the same age-gender-based funding as practices serving wealthy, healthy Pākehā populations.
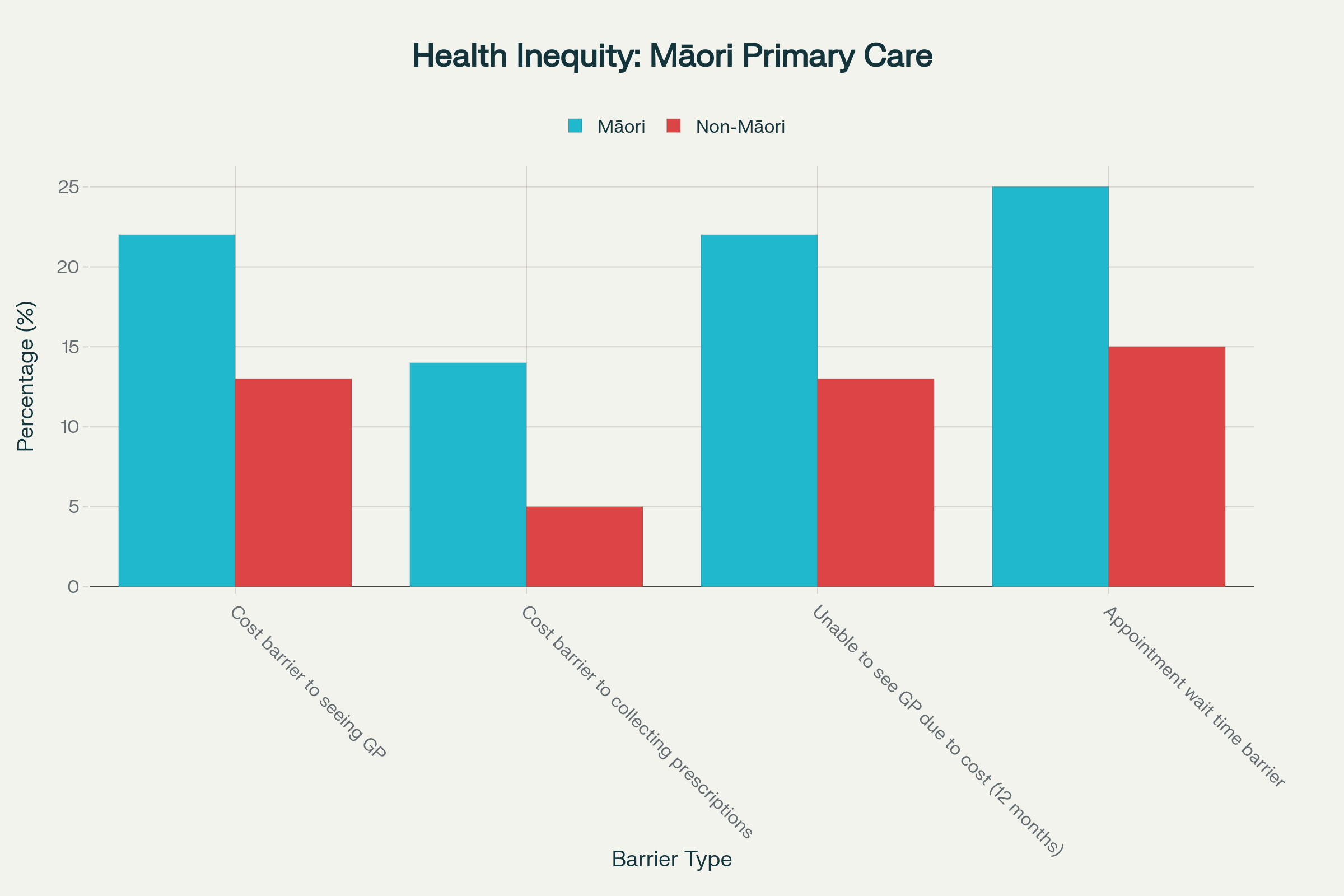
Māori experience significantly higher barriers to accessing primary healthcare, with twice the rate of cost barriers to collecting prescriptions compared to non-Māori - a direct result of systemic underfunding and colonial health policy design
The Issue That Matters
Here is what Derek Cheng’s article deliberately obscures: Māori experience 22 percent cost barriers to seeing a GP compared to 13 percent for non-Māori. Māori face cost barriers to collecting prescriptions at nearly three times the rate of non-Māori - 14 percent versus 5 percent. Māori children aged 12-24 months experience barriers to seeing a GP at 8.3 percent compared to 2.8 percent for New Zealand European children. These are not unfortunate statistics - they are the inevitable outcomes of a funding system designed by colonisers for colonisers.
The article quotes Dr Angus Chambers of GenPro saying practices are “really squeezed” and describing a “vicious cycle” where underfunding forces fee increases, which delays care and increases emergency department presentations. It quotes Dr Bryan Betty citing international research showing “$1 invested in primary care returns approximately $8 to $14”. These moderate professional voices provide cover for what is actually happening: a deliberate policy of starving public primary care to create the conditions for privatisation.
Labour’s Dr Ayesha Verrall - whose credentials as an infectious diseases physician are deployed to legitimise the proposal - suggests creating an “Independent Pricing Authority” to depoliticise funding decisions. The article presents this as potentially addressing “a $137 million net income deficit” identified in the 2022 Sapere report that showed general practice makes a 7.6 percent loss each year.
But notice what the article never mentions: the Waitangi Tribunal’s definitive finding that the Crown breached Te Tiriti o Waitangi by failing to design and administer the primary health care system to actively address persistent Māori health inequities. Notice it never mentions the calculated $531 million in cumulative losses for Māori providers serving 332,051 enrolled Māori patients between 2003-2018. Notice it never mentions the finding that proper investment in “by Māori for Māori” primary healthcare should be $1 billion per year, and the cost of NOT making this investment has been $5 billion annually.
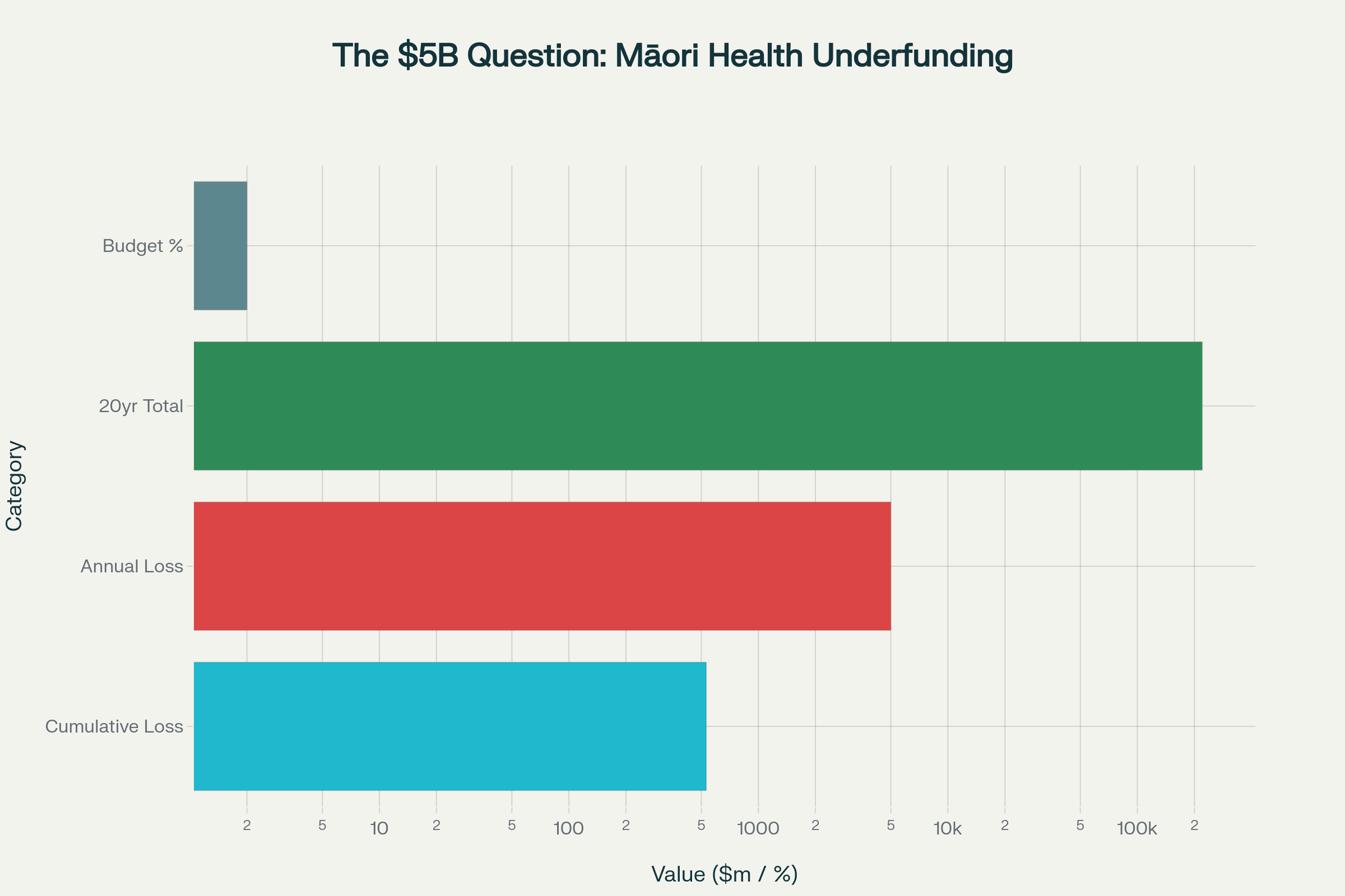
Independent analysis reveals Māori health providers have been systematically underfunded by over $500 million since 2003, contributing to an estimated annual health loss valued at $5 billion in 2018 - while Māori providers receive only 2% of the total health budget
The Colonial Architecture of Healthcare Apartheid
Derek Cheng, described by the Herald as someone who “values holding those in power to account and shining a light on issues kept in the dark”, has produced an article that does precisely the opposite. By framing this as a technical policy debate about funding mechanisms and “fish hooks,” Cheng obscures the fundamental reality: New Zealand’s primary care system is a colonial structure that systematically produces Māori death and disability while enriching private capital.
The article’s “both sides” approach - giving equal weight to GPs who say they’re underfunded and a Government minister who claims funding is adequate - creates false balance. Cheng presents this as a legitimate policy position rather than what it is: gaslighting from a far-right Christian fundamentalist whose government has - https://www.wsws.org/en/articles/2025/01/24/dyvv-j24.html. systematically attacked Māori health institutions, abolished Te Aka Whai Ora (the Māori Health Authority), slashed Kaupapa Māori services funding, and pushed “record investment” claims while the Waitangi Tribunal found these actions constitute further Treaty breaches.
The article quotes Chambers expressing caution about Labour’s proposal, saying “if it was stacked with political appointees, we would not see it as a good system”. This concern about “political appointees” is rhetorical sleight of hand - the current system is entirely controlled by political decisions, made by politicians who have overseen decades of systematic underfunding. An independent authority could hardly be worse than the status quo where government funding has fallen short of cost pressures 10 times in the past 20 years.
But here is the deeper deception: Labour’s proposal explicitly states the authority “wouldn’t change how fees are set or reviewed” and practices “could still ask to have their fees looked at”. This means patient co-payments would continue, the two-tier system would continue, and the cost barriers that force 22 percent of Māori to delay or forego GP care would continue. Verrall’s careful phrasing - “not pushing for abolishing or fixing” patient fees - reveals Labour’s fundamental unwillingness to challenge the neoliberal funding model that generates inequity.
The Neoliberal Consensus and Privatisation by Stealth
Both major parties agree on the core premise: primary care should remain a quasi-privatised system where GPs operate as small businesses, patients pay significant co-payments, and government funding serves as a subsidy rather than full public provision. This model was introduced with the 2001 Primary Health Care Strategy and has been maintained under both Labour and National governments.
The article notes that Chambers expresses caution about fixed patient fees, saying they “usually fund it reasonably well to get people on board, and then, slowly but surely, it withers on the vine”. He adds that free visits lead people to “undervalue the service” and cites prescription charges as making patients “more careful with their medicines”. This victim-blaming rhetoric - suggesting Māori who cannot afford healthcare are simply careless - is presented without challenge by Cheng.
Meanwhile, the Coalition Government is aggressively pursuing privatisation of secondary care, with Health Minister Simeon Brown directing Health NZ to give private hospitals 10-year outsourcing contracts for elective surgeries, claiming this will “improve cost effectiveness” and “provide clear investment signals” to the private sector. The government is also exploring Public-Private Partnerships where private companies could build and potentially operate public hospitals.
This privatisation strategy directly contradicts international evidence showing higher rates of privatisation correspond with poorer health outcomes. Yet Cheng’s article presents Labour’s Independent Pricing Authority as the alternative, when in fact Labour’s proposal accepts and reinforces the same privatised structure.
The Role of Corporate Media in Manufacturing Consent
The New Zealand Herald is owned by NZME, a publicly-listed media conglomerate that has faced sustained criticism for its editorial direction and recent shareholder battles involving billionaire Jim Grenon. Grenon, who acquired a 9.3 percent stake in NZME and immediately moved to replace most of the board with his own nominees, has stated that “editorial content is a side issue” and promised an “emphasis on factual accuracy, less selling of the writer’s opinion and appealing to a wider political spectrum” - language that echoes the “objectivity” rhetoric used to neutralise progressive journalism globally.
Derek Cheng’s article perfectly exemplifies this manufactured objectivity. By presenting a policy debate divorced from its colonial context, by giving equal weight to those perpetuating health inequity and those suffering it, by never mentioning Te Tiriti obligations or the Waitangi Tribunal findings, Cheng produces journalism that serves power while claiming to scrutinise it.
The article’s headline - “Fish hooks and cautious support: GPs weigh up Labour’s new health policy” - frames this as a technical question of policy mechanics rather than what it is: a life-or-death question of whether New Zealand will finally honour Te Tiriti obligations and fully fund equitable healthcare, or continue the colonial project of Māori health dispossession.
Labour’s Historic Betrayal and Complicity
The article notes that Chambers says “Labour’s got a track record of doing this too - significant underfunding, and when they were in a position to do something about it, they didn’t”. This is one of the few moments of truth in the entire piece. Labour governed from 2017-2023 with an absolute majority from 2020-2023, and during this time continued the systematic underfunding of Māori healthcare while spending over $220 billion on health with “little measurable improvement to Māori health outcomes”.
Labour established Te Aka Whai Ora in 2022 as a response to the Waitangi Tribunal’s damning findings, but the authority was given insufficient funding and power to effectively address the systemic inequities. The Coalition Government abolished Te Aka Whai Ora in February 2024, and the Waitangi Tribunal has now found this disestablishment constitutes further Treaty breaches.
Labour’s current proposal for an Independent Pricing Authority is positioned as “learning from mistakes,” but it maintains the same fundamental structure that generates inequity. is meaningless when the proposal explicitly maintains patient co-payments and the privatised funding model (https://www.nzherald.co.nz/nz/politics/fish-hooks-and-cautious-support-gps-weigh-up-labours-new-health-policy/FVMSDWUOQJGTTOMXQOWER5LXQA/).[]
The True Cost of Colonial Healthcare
The Waitangi Tribunal found that over $200 billion has been spent on health since 2012, yet Māori health outcomes have barely improved. Of the $907 million in capitation funding for primary health providers in 2017/18, only $28.7 million (3.1 percent) went to Māori services, despite Māori being disproportionately represented in high-needs groups.
The life expectancy gap between Māori and non-Māori remains 6.4 years for men and 5.5 years for women. Māori children are more than twice as likely to be diagnosed with asthma and more than 40 times more likely to be hospitalised with acute rheumatic fever than Pākehā children. Māori experience worse survival rates for 23 out of the 24 most common cancers. When Māori do access healthcare, the quality of care provided is systematically lower than for non-Māori.
These are not accidents. They are not unfortunate outcomes of resource constraints. They are the direct, predictable, intentional results of a colonial health system designed to extract resources from Māori communities while providing inadequate care. The current capitation model actively discriminates against Māori by failing to account for the higher health needs, the historical underutilisation due to cost barriers, and the structural barriers that Māori patients face.
The Māori Values Framework for Health Justice
As kaitiaki, we must ground our analysis in Māori values and spirituality to understand what true health equity requires. Hauora - holistic wellbeing encompassing physical, mental, spiritual, and family health - cannot be achieved through a system that treats healthcare as a commodity. Whakapapa - the connections between people, land, and ancestors - is disrupted when Māori cannot access affordable care in their own communities and must travel to urban centers or delay treatment.
Manaakitanga - the ethic of care and hospitality - demands that healthcare be provided with generosity and respect, not rationed based on ability to pay. Tino rangatiratanga - self-determination and sovereignty - requires that Māori have genuine authority over healthcare policy and funding decisions, not token consultation.
The Waitangi Tribunal explicitly found that the primary health care framework does not “recognise and properly provide for tino rangatiratanga and mana motuhake of hauora Māori”. Labour’s Independent Pricing Authority, controlled by “financial and commercial knowledge” as Chambers demands, would continue this violation of tino rangatiratanga by placing technical expertise above Māori authority.

The Māori Green Lantern Fighting Misinformation And Disinformation From The Far Right
The Path Forward: Abolition Not Reform
The solution is not an Independent Pricing Authority. The solution is not modest funding increases that still leave practices running at a loss. The solution is the complete abolition of the neoliberal primary care model and the establishment of a fully publicly funded, universally accessible, zero-cost-at-point-of-care system that prioritises Māori health equity.
This means:
- Eliminating all patient co-payments for primary care consultations and prescriptions
- Fully funding the $1 billion annual investment required for “by Māori for Māori” primary healthcare
- Paying the $531 million in compensation owed to Māori providers for decades of systematic underfunding
- Establishing genuine Māori authority over health policy and funding through reinstatement of Te Aka Whai Ora with real power and resources
- Employing GPs and primary care staff as salaried public employees with equitable pay, regular benefits, paid continuing education, and collective bargaining rights
- Ending the privatisation agenda and returning all outsourced elective surgeries and specialist care to properly funded public facilities
- Redesigning the capitation formula to explicitly account for ethnicity, multimorbidity, socioeconomic deprivation, and structural barriers to care
Research consistently shows that for every $1 invested in primary care, the return is between $8 and $14 in avoided hospital costs. The current system where 33 percent of GP practices have closed their books to new patients, forcing 290,000 New Zealanders to rely on emergency departments for primary care, is economically irrational as well as morally bankrupt.
The Real Bottom Line
Derek Cheng’s article in the New Zealand Herald is not journalism - it is propaganda that naturalises health inequity and prepares the public to accept continued Māori suffering as inevitable. By focusing on technical policy mechanisms while ignoring the Waitangi Tribunal findings, the scale of Māori underfunding, and the government’s privatisation agenda, Cheng produces content that serves the colonial state and corporate capital.
NZME, under pressure from billionaire shareholders who explicitly want to shift editorial direction away from progressive coverage, has every incentive to frame health policy as a question of fiscal responsibility rather than colonial violence. Simeon Brown, a fundamentalist Christian with deep ties to conservative Baptist churches that actively place members in political positions, has every incentive to maintain a system that preserves wealth and power for Pākehā while blaming Māori for their own poor health outcomes.
And Labour, terrified of challenging neoliberal orthodoxy and alienating middle-class Pākehā voters, offers symbolic reforms that change nothing fundamental while claiming to address the concerns of Māori health advocates.
The cost of this collective failure is measured in Māori lives lost, Māori children suffering preventable illness, Māori elders choosing between food and prescriptions, and the continued violation of Te Tiriti o Waitangi that forms the constitutional foundation of this nation.
We deserve better. Our tūpuna demand better. Our mokopuna require better. And we will fight until the colonial healthcare system is dismantled and replaced with a system grounded in manaakitanga, tino rangatiratanga, and the fundamental principle that healthcare is a human right, not a commodity to be rationed by ability to pay.
Kia kaha. Kia māia. Kia manawanui.
If you have found value in this analysis and wish to support this kaupapa, please consider a koha to HTDM: 03-1546-0415173-000. I understand these are tough economic times for many whānau, so please only contribute if you have the capacity and genuinely wish to do so.
Nāku noa, nā
The Māori Green Lantern