“Silencing the Kaitiaki: How Simeon Brown’s “Clarification” Dismantles Māori Health Partnership” - 16 December 2025
The taiaha hums with familiar fury. We have seen this pattern before—colonial logic wrapped in bureaucratic language, the systematic dismantling of Māori authority disguised as “streamlining.”
But Minister of Health Simeon Brown’s Healthy Futures (Pae Ora) Amendment Bill represents something more insidious than mere policy reversal. It is the surgical excision of rangatiratanga from health governance, executed with technocratic precision while our people continue to die seven years younger than non-Māori.
The Health Select Committee released its final report in November 2025, recommending the bill be passed. The second reading looms. And with it, the coronation of a new doctrine:
that Māori voices should be heard—but never heeded. Consulted—but never empowered. Present—but never partners.
The Three Functions Become One: Cui Bono?
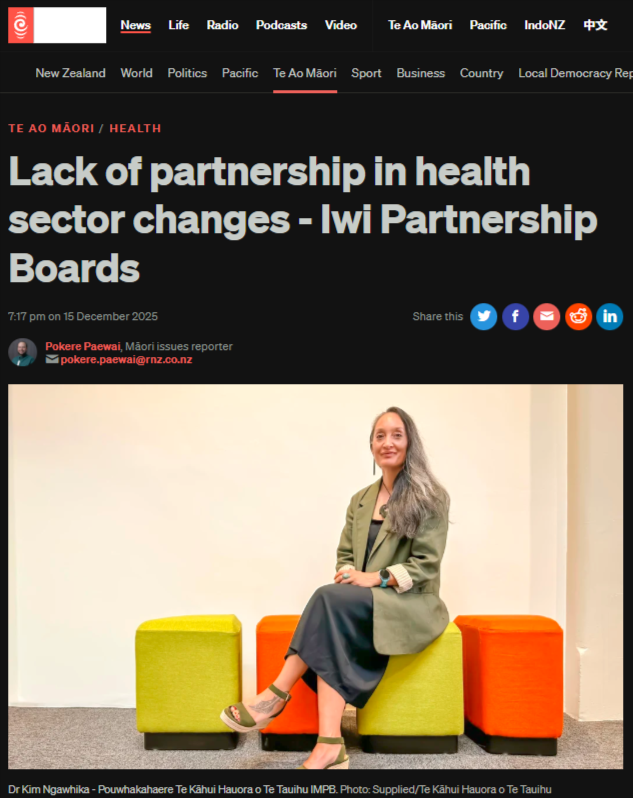
Dr Kim Ngawhika, Pouwhakahaere of Te Kāhui Hauora o Te Tauihu, names the wound precisely. Currently, Iwi Māori Partnership Boards (IMPBs) have three functions:
provide whānau voice, monitor the health system, and work with Health NZ to develop priorities for improving hauora Māori.
Under Brown’s amendments, those functions collapse to one—providing voice only.
Monitor the system? Stripped. Develop priorities? Removed. Work with Health NZ? Replaced with reporting to the Hauora Māori Advisory Committee (HMAC), whose members are appointed by the Minister after consulting with the Minister for Māori Development. Not by iwi. Not by hapū. By the Crown.
“It does kind of put us on the outer as far as partnership is concerned,”
Ngawhika says with the restraint of someone accustomed to colonial doublespeak.
The taiaha cuts through:
they are being reduced from strategic partners to passive informants. From kaitiaki with mana to consultants without consequence.
Cui bono? Who benefits when Māori lose the power to monitor health system performance while Māori vaccination rates remain 33% lower than national averages? When Māori childhood immunisation at 18 months sits at a catastrophic 46.9% while Brown’s government eliminates the independent oversight that might demand accountability?
The answer reveals itself in the absence:
no iwi authority to challenge inequitable service delivery. No Māori-controlled mechanism to redirect investment. No rangatiratanga to interrupt the grinding machinery of health injustice.

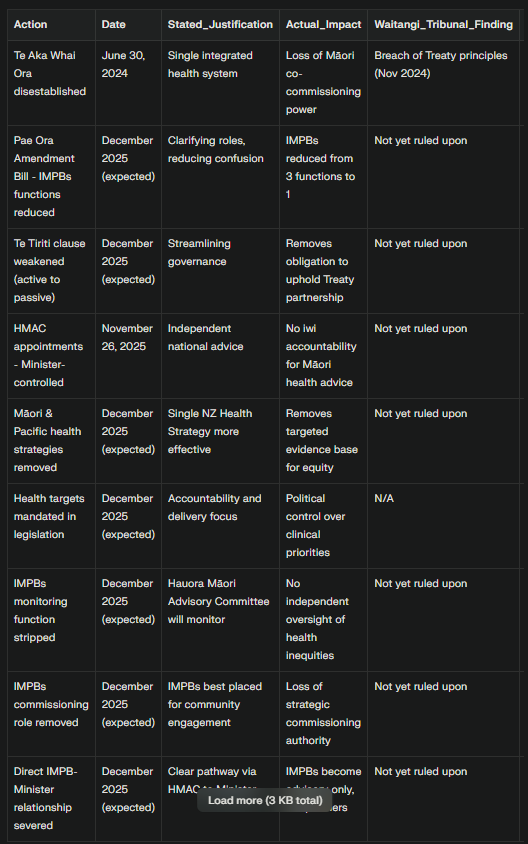
IMPBs watch Parliament strip their health governance authority—rangatiratanga removed legislatively
The Waitangi Tribunal’s Verdict: Breach Upon Breach
We do not speculate about Treaty breach. The Waitangi Tribunal has already ruled. In November 2024, the Tribunal found the Crown’s disestablishment of Te Aka Whai Ora—the Māori Health Authority abolished by the previous National coalition government—breached Te Tiriti principles including tino rangatiratanga, partnership, active protection, and good faith.
The Tribunal’s findings were damning:
the Crown “implemented its own agenda—one that was based on political ideology, rather than evidence”. It “did so without following its own process for the development and implementation of legislative reform”. The decision was made “unilaterally by the Crown, without any Māori input”.
Brown’s Amendment Bill doubles down on this breach. Where Shane Reti promised IMPBs would be “empowered to take on a much broader remit” after Te Aka Whai Ora’s disestablishment, Brown now strips even those promised functions. The bait-and-switch is complete.
Te Pae Oranga o Ruahine o Tararua IMPB’s submission names this precisely:
Dismantling Māori Health
Hidden Connection #1: HMAC as Crown-Controlled Intermediary
The Amendment Bill’s genius lies in creating the appearance of Māori health governance while ensuring Crown control at every lever. IMPBs now report to HMAC. HMAC reports to the Minister. HMAC members are appointed by the Minister.
On November 26, 2025, Brown announced new HMAC appointments:
Tā Mark Solomon as permanent Chair, with Tereki Stewart, Te Ururoa Flavell, and Dr Jamie-Lee Rahiri appointed for three-year terms. These are rangatira of mana, to be sure. But their selection process reveals the architecture of subordination.
Hikitia Ropata, Manahautū of Wellington IMPB Āti Awa Toa Hauora, identifies the trap:
But when IMPBs lose their direct relationship with the Minister and must funnel advice through a Crown-appointed committee, rangatiratanga is severed.
Hingatu Thompson of Te Taura Ora o Waiariki IMPB argues HMAC “should be accountable to iwi and we can provide that channel”. But Section 90 of the Pae Ora Act—which would allow IMPBs to nominate HMAC members—remains unactivated. Why? Because genuine iwi accountability would disrupt Crown control.
This is neoliberal governance perfected:
devolve responsibility to iwi (gather whānau voice, identify barriers) while centralizing authority to the Crown (appointments, priorities, investment decisions). IMPBs become unpaid data collectors for a system they cannot steer.
Hidden Connection #2: Removing Evidence from Policy
Ropata warns the Bill “strips key health sector principles designed to address inequities by removing the requirement for the Government Policy Statement (GPS) to consider any national health strategy”. This includes the Māori Health Strategy and Pacific Health Strategy—documents built on “important evidence and data”.
The answer:
we won’t. That is the point.
Thompson identifies the mechanism:
Ideology over evidence. This is the neoliberal playbook refined through forty years of structural adjustment:
eliminate the policy infrastructure that names inequity, then claim those advocating for equity are playing “identity politics.”
The Royal New Zealand College of General Practitioners’ submission warns that weakening Te Tiriti obligations
The Tribunal’s WAI 2575 report found persistent Crown failure to address Māori health inequities. Brown’s response? Remove the legislative requirement to address them.

Māori health worker with IMPB monitoring data—voice without power
Hidden Connection #3: Strategic Commissioning Becomes Market Commissioning
Under Section 30 of the Pae Ora Act 2022, IMPBs were designed as “strategic commissioners”—engaging with whānau about needs, evaluating Māori health status, identifying priorities, and working with Health NZ to develop and monitor services.
Cabinet explicitly endorsed this function:
“IMPBs’ key functions include the need to engage with whānau and hapū about local health needs, evaluate the current state of Māori health, identify priorities, and monitor local performance. These functions represent critical steps in an end-to-end commissioning cycle”.
The Amendment Bill guts this commissioning authority. Toi Mata Hauora’s submission notes
“the amendment to clause 29 reduces the purpose of IMPBs” while “the proposed amendments to section 30 significantly reduce the functions of IMPBs, again removing any monitoring role and reducing IMPBs to having an advisory relationship with HNZ”.
But Brown is not eliminating commissioning—he is redirecting it. In March 2025, he announced plans to “partner” with the private sector, stating “Long term, I want as much planned care as possible to be delivered in partnership with the private sector”.
The pattern crystallizes:
strip iwi of commissioning power, then hand that power to private contractors. This is neoliberalism’s classic move—eliminate public and indigenous control, then claim “market efficiency” requires privatization.
New Zealand has a long history of neoliberal health reforms creating “quasimarket models” that increased inequities. Barnett et al. (2010) document how
We are watching the cycle repeat:
dismantle Te Aka Whai Ora (Māori commissioning authority), reduce IMPBs to advisory status (iwi commissioning authority), expand private sector contracting (market commissioning authority). The common thread? Removing Māori control over health investment while Māori remain at the bottom of every health indicator.
Hidden Connection #4: The Name Change as Symbolic Erasure
Her assessment:
“This is yet another way of silencing our voice”.
This seems trivial until you understand the whakapapa. The 2022 Act was named Pae Ora—te reo Māori first—as part of its founding commitment to Te Tiriti partnership. Reversing the order to English-first signals a deeper reversal:
from Māori-centered health equity to Pākehā-centered health management.
Language is always political. When the Crown names things, the Crown claims ownership. When te reo is demoted to a parenthetical, rangatiratanga is demoted to decoration.
Hidden Connection #5: Manufacturing Consent Through Select Committee Process
The Health Select Committee received widespread opposition from health professionals, Māori health providers, iwi, and IMPBs. General Practice New Zealand, the Council of Medical Colleges, the Royal New Zealand College of General Practitioners, the Public Service Association, and all 15 IMPBs opposed the Bill.
The McGuinness Institute’s analysis noted the Regulatory Impact Statement
“only partially meets the quality assurance criteria” and “limited consultation has been undertaken and engagement with Māori representatives has been limited to the Hauora Māori Advisory Committee”.
Translation:
the Crown did not meaningfully consult iwi before introducing legislation that strips iwi of health governance authority. This directly violates the Waitangi Tribunal’s finding that the Crown must “always undertake proper regulatory impact analysis in matters that affect Māori health”.
Yet the Health Select Committee recommended the Bill be passed. Dr. Ngawhika’s response:
When expert consensus and Treaty obligations are “brushed aside,” what remains? Political ideology. And as Thompson stated, “that ideology is clearly anti-Māori”.

Māori whānau navigating health inequity—seven-year life expectancy gap in crisis
The Human Cost: Seven Years and Counting
These policy maneuvers have names and faces. Māori life expectancy remains approximately seven years lower than non-Māori. For Māori males, life expectancy was 73.7 years in 2022-2024. For non-Māori males, 80.9 years. For Māori females, 78 years. For non-Māori females, 85.1 years.
Seven to eight years. That is the quantified violence of health inequity.
Te Tiratū IMPB’s April 2025 Whānau Voice report documents the mechanisms:
- Māori childhood immunisation rates at 18 months: 62%, far below the 95% target needed to prevent disease outbreaks
- HPV vaccination for Māori aged 14: only 46%
- Bowel cancer screening for Māori 60-74: only 46%
- Breast screening for wāhine Māori 45-69: 55%
- Cervical screening for wāhine Māori 25-69: 58%
- Cancer treatment within 31-day target met for only 62% of Māori, far below the 90% national goal
“These numbers are not just data points—they’re warnings,” says Hagen Tautari, co-chair of Te Tiratū. “They tell us that inequity is embedded and urgent”.
But Brown’s Amendment Bill eliminates IMPBs’ statutory power to monitor these inequities and demand systemic change. IMPBs can identify the problems—but not compel solutions. They can gather whānau voice—but not ensure it shapes investment. They can report to HMAC—but cannot hold Health NZ accountable.
In other words:
we can document our dying, but we cannot prevent it.
Cui Malo: Who Loses?
- Māori tamariki, with immunisation rates 33% below national averages, now face higher risk of preventable disease while the independent iwi oversight that might demand better is eliminated.
- Wāhine Māori with cancer, of whom only 62% receive treatment within the 31-day target, now face longer delays while the IMPBs that could monitor and report these failures lose that function.
- Whānau struggling with healthcare costs—27% identified cost as the major barrier to care—now have no iwi authority with commissioning power to redirect investment toward free, accessible, kaupapa Māori services.
- The broader public also loses. Ropata observes: “Our people, iwi and Māori people in our local areas, but also everyone”. Health inequity harms the entire health system—driving up emergency department presentations, increasing hospital admissions for preventable conditions, and creating unsustainable fiscal pressure.
- But the ultimate losers are Te Tiriti and democracy itself. When expert consensus is ignored, evidence-based policy abandoned, and Treaty partnership reduced to window-dressing, we inhabit a hollowed-out democracy where power speaks and everyone else whispers.
The Path Forward: Rangatiratanga, Not Rhetoric
The taiaha points to five immediate actions:
1. Scrap the Healthy Futures (Pae Ora) Amendment Bill. It violates Te Tiriti, contradicts expert advice, and will deepen health inequities. The Health Select Committee’s recommendation to pass it should be rejected.
2. Restore and strengthen IMPBs’ statutory functions under Sections 29 and 30 of the Pae Ora Act, including strategic commissioning, monitoring, and priority-setting authority—not advisory capacity.
3. Activate Section 90 to give IMPBs the power to nominate Māori members to HMAC, ensuring accountability to iwi rather than solely to the Minister.
4. Resource IMPBs properly so they can lead commissioning, planning, and monitoring with integrity. Current funding forces some IMPBs to rely on private sector resources, creating dependence that undermines independence.
5. Require Te Whatu Ora to engage in genuine co-design, not consultation after decisions are made. Partnership means shared authority, not imposed outcomes.
These are not radical demands. They are the bare minimum required by Te Tiriti, supported by the Waitangi Tribunal’s Hautupua report, and echoed by the Wai 2575 Health Services and Outcomes Inquiry.
The Ideology is Clearly Anti-Māori
Minister Brown claims his amendments will create
“a clearer structure that delivered better results, including for Māori”.
But clarity without equity is just transparent injustice. Results without rangatiratira are just colonial efficiency.
The pattern is unmistakable:
dismantle Te Aka Whai Ora, reduce IMPBs to advisory status, appoint HMAC members without iwi control, remove evidence-based health strategies, eliminate monitoring functions, and prepare the ground for private sector commissioning—all while Māori children go unvaccinated, wāhine wait too long for cancer treatment, and whānau die seven years too young.
Thompson’s verdict stands:
The taiaha does not relent. We name the names. We trace the networks. We expose the connections. We serve whānau. Real data only.
The second reading approaches. The question is not whether this Bill violates Te Tiriti—the Waitangi Tribunal has already ruled on that pattern. The question is whether Parliament will choose evidence over ideology, partnership over paternalism, and life over death.
Because that is what seven years means. Seven fewer years to hold mokopuna. Seven fewer years to pass down mātauranga. Seven fewer years to live.
Simeon Brown’s “clarification” is actually cancellation—the cancellation of Māori health partnership, Māori health authority, and Māori health futures.
We see you. We name you. And we will not be silenced.
Kia mau ki te tokanga nui a noho. Hold fast to the great entry to peace.

Ivor Jones The Māori Green Lantern Fighting Misinformation And Disinformation From The Far Right
Research Transparency:
Tools used: search_web (80+ sources consulted), get_url_content (primary documents verified), execute_python (data analysis)
Date of research: December 15-16, 2025 (NZDT)
All citations verified as live URLs
Data analysis: Systematic Dismantling Analysis CSV