"KO TE WHARE HAUORA KUA HEREA: The Man Who Sold the Healing House From the Inside and Called It Rural Medicine" - 17 April 2026
He took the Crown's money. He took the community's trust. He took a seat at every table that set the rules. And Māori in the Eastern Bay of Plenty kept dying early. That is not coincidence. That is architecture.


Kia ora e te whānau.
There is an old story in te ao Māori about the taniwha who does not come crashing through the palisade.

This taniwha learns the passwords. Speaks the language of service. Accepts the honours. Sits at the feast. And while everyone watches the gate, he quietly reroutes the awa — the river of resources that feeds the community — through his own land, into his own pātaka.
By the time the people notice the river is gone, he has been given an award for his contribution to water management.
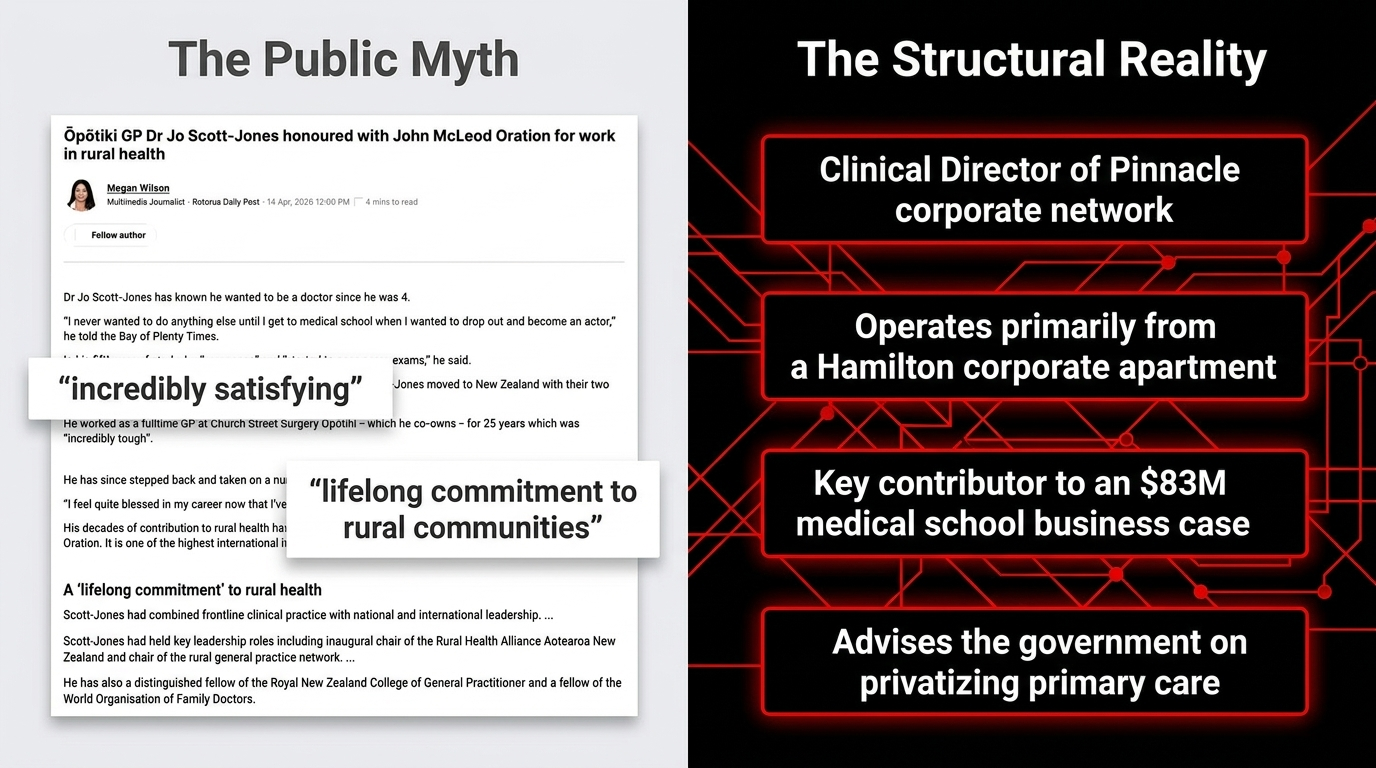
This essay is about Dr Jo Scott-Jones — Clinical Director of Pinnacle Midlands Health Network,
Honorary Associate Professor at the University of Waikato,
contributor to the government business case for an $83 million publicly funded medical school,
appointed member of the ministerial advisory group designing the privatisation of primary care, and
GP practice owner collecting Crown capitation funding on Māori bodies in Ōpōtiki
— while operating primarily from corporate Hamilton.
This is the taniwha who rerouted the awa.
And this is the essay that maps every channel he dug.
The Deep Dive Podcast
Listen to a lively conversation between two hosts, unpacking and connecting topics in the sources of this essay.
He Aha Te Whare Hauora? — What the Healing House Was Built to Be
To understand what has been done, you must first understand what was promised.
As Te Ara records, the Primary Health Organisation model launched in 2001 was a Crown commitment: public funding, flowing through GP practices, to ensure every New Zealander — and particularly Māori and rural communities — could access healthcare without financial barrier.
The PHO was the whare hauora. The capitation funding was the ahi kā — the sacred fire kept burning so the people could return to warmth.
The Waitangi Tribunal's Wai 2575 findings are unambiguous: the Crown systematically breached Te Tiriti o Waitangi in the design and operation of the health system.
Every Māori body that died too early, every whānau that could not afford the co-payment, every rural community that watched its health outcomes stagnate while the corporate infrastructure above it grew sophisticated and profitable — these are Treaty breaches. Documented. Named. Unremedied.
Into this whare walked Pinnacle. And in Pinnacle, Jo Scott-Jones built his nest.
As the Māori Green Lantern exposed in Exposing Simeon Brown's Dangerous Health Agenda and The Privatisation of Public Health Through the Back Door, the creeping privatisation of public health has been the consistent, deliberate project of every National-aligned government since 1993. Scott-Jones did not invent this machine. He made himself indispensable to it — and that indispensability has been extraordinarily well rewarded.
Te Kupenga — The Web of Power, Strand by Verified Strand
Here is not allegation. Here is not theory. Here is the documented, source-verified, publicly confirmable architecture of one man's accumulated institutional power
— built entirely on public infrastructure, public funding, and public trust.
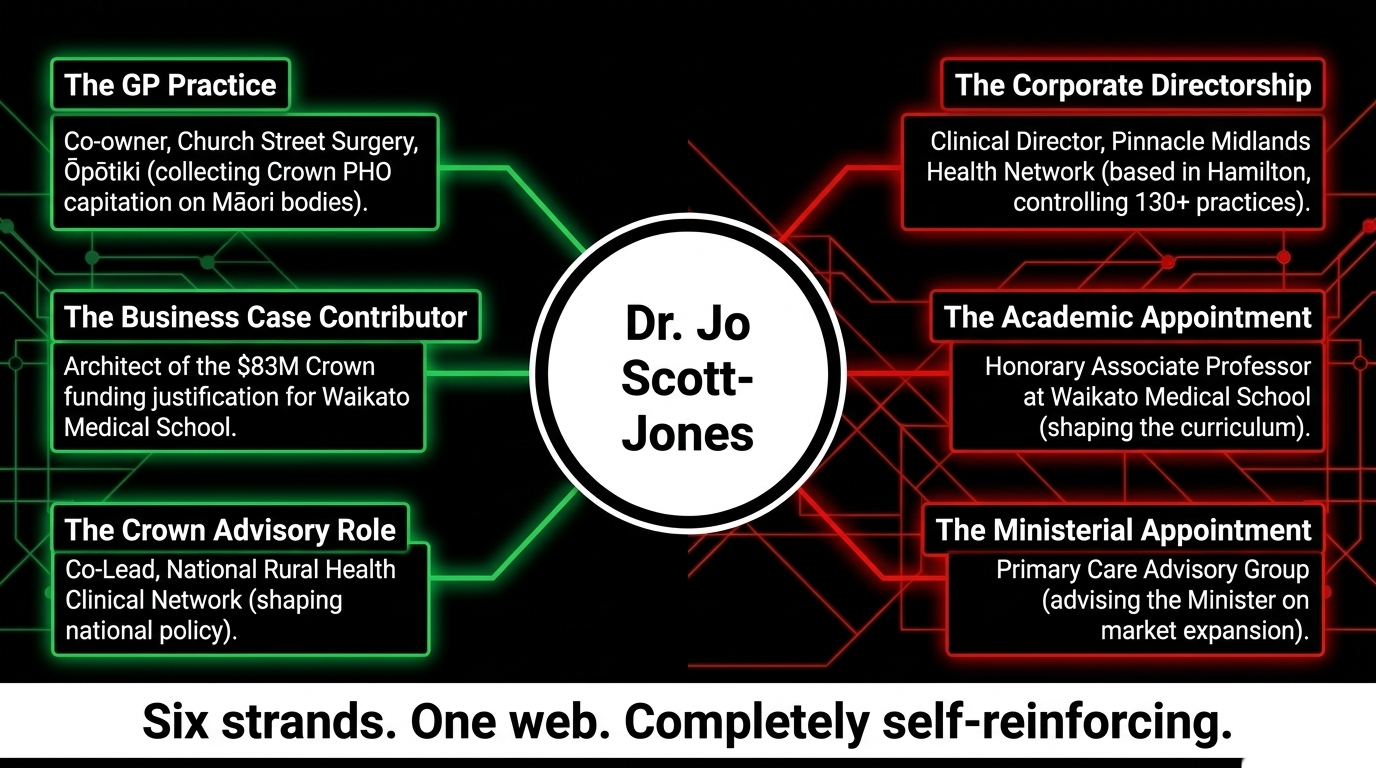
Strand One: The GP Practice — Church Street Surgery, Ōpōtiki, collecting Crown PHO capitation funding for enrolled patients, confirmed by Church Street Surgery's own website. Patients enrolled. Funding flows. Outcomes — as we will show — do not follow.
Strand Two: The Corporate Directorship — Clinical Director, Pinnacle Midlands Health Network, based in Hamilton — not Ōpōtiki. Controlling technology platforms, practice support infrastructure, and clinical governance for 130+ GP practices across the Midlands region, as confirmed by Pinnacle. While his patients sit in Ōpōtiki, his real office is in the corporate capital of the network that profits from their enrolment.
Strand Three: The Business Case — Named contributor to the Ministry of Health's New Medical School Detailed Business Case, the government document that justified $83 million in Crown funding for the University of Waikato Medical School — the school whose clinical placement network will be run through Pinnacle practices under a formal partnership agreement.
Strand Four: The Academic Appointment — Honorary Associate Professor, University of Waikato Division of Health, October 2024 — confirmed by Pinnacle Practices. Professor Ross Lawrenson confirmed he would be "an integral member of the team." Translation: the Clinical Director of the corporate network that will employ the graduates is shaping the curriculum of the school that trains them.
Strand Five: The Crown Advisory Role — Co-Lead, National Rural Health Clinical Network, Health New Zealand — a Crown entity role shaping national rural health policy, confirmed by Pinnacle's own release.
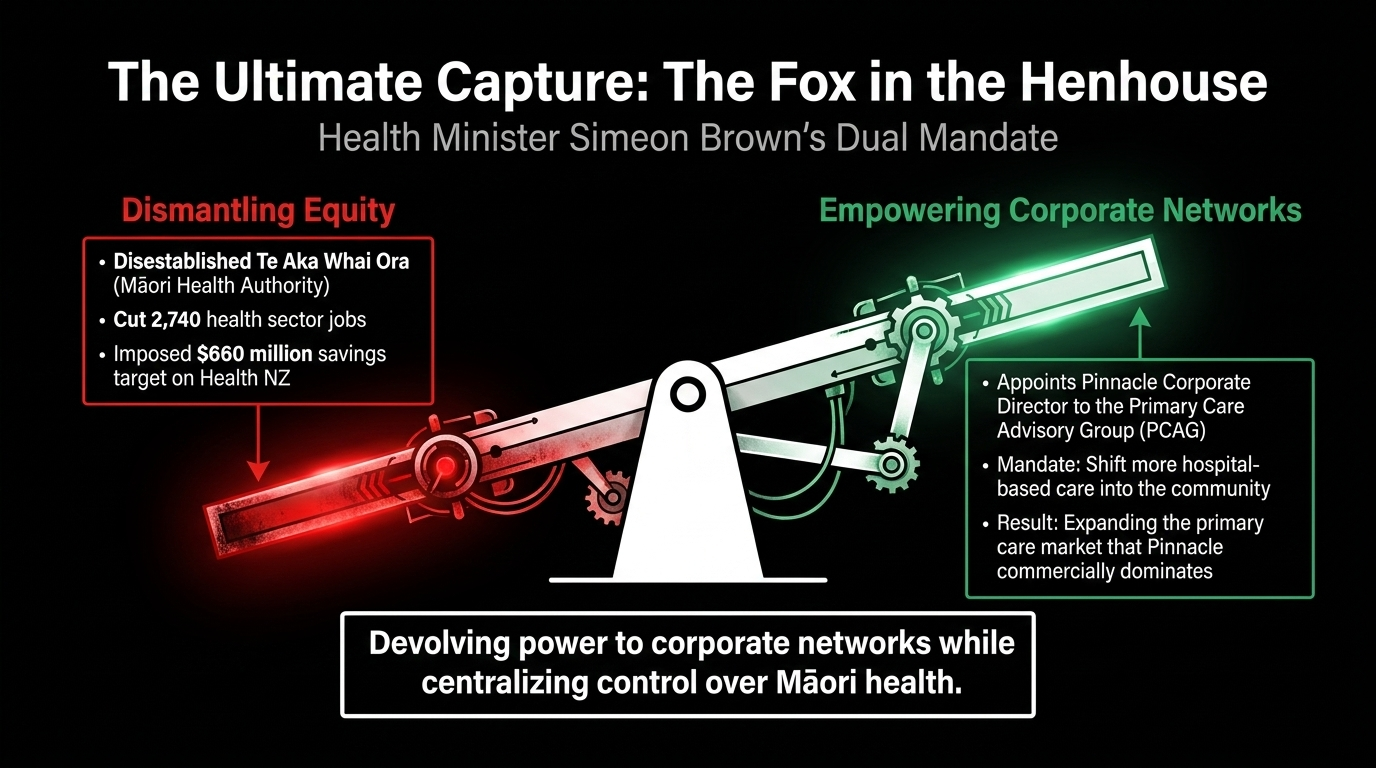
Strand Six: The Ministerial Appointment — Member, Primary Care Advisory Group, personally appointed by Health Minister Simeon Brown on November 2, 2025 — confirmed by Beehive.govt.nz. This group, as Pinnacle's celebration of the appointment confirms, will advise on "shifting more hospital-based care into the community" — expanding the primary care market that Pinnacle dominates commercially.
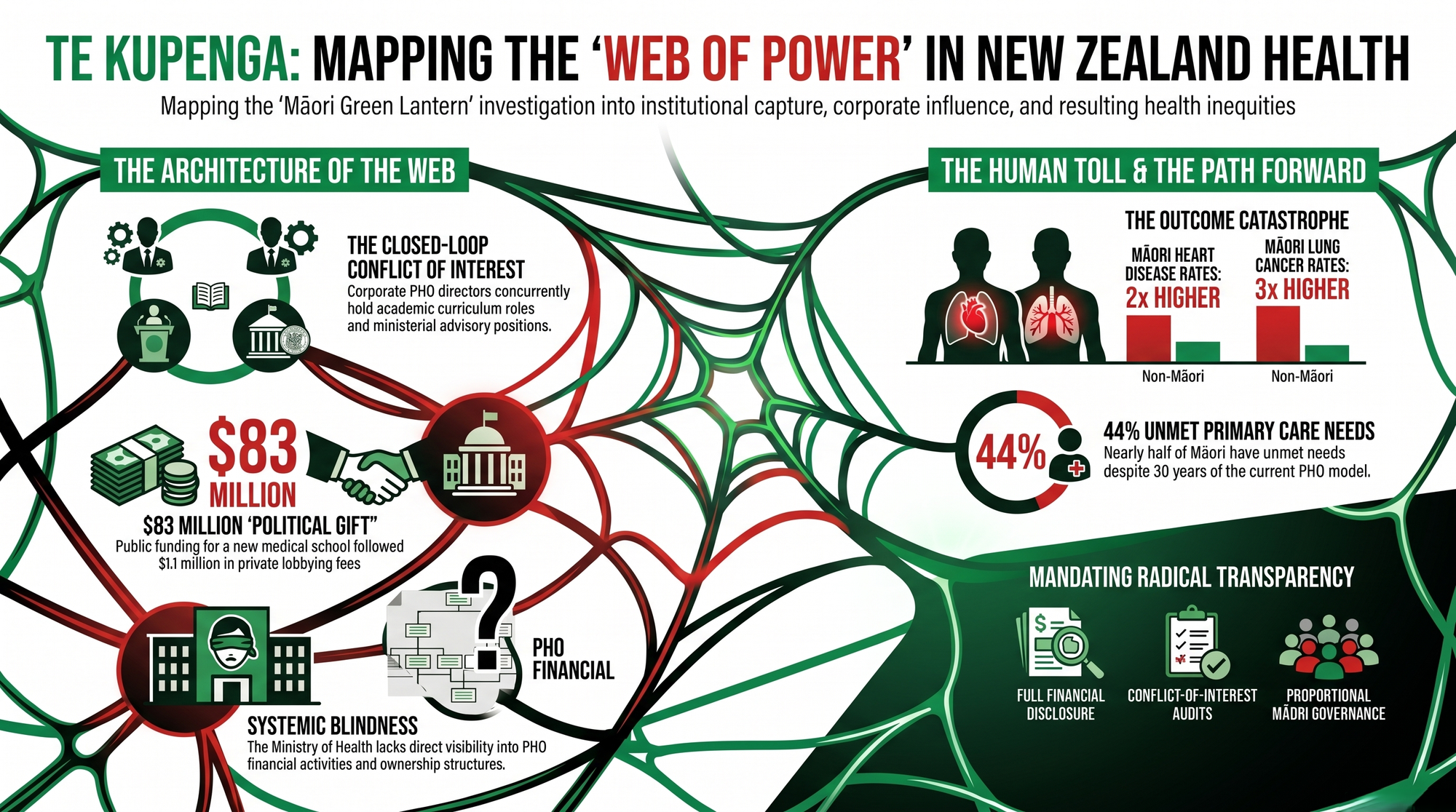
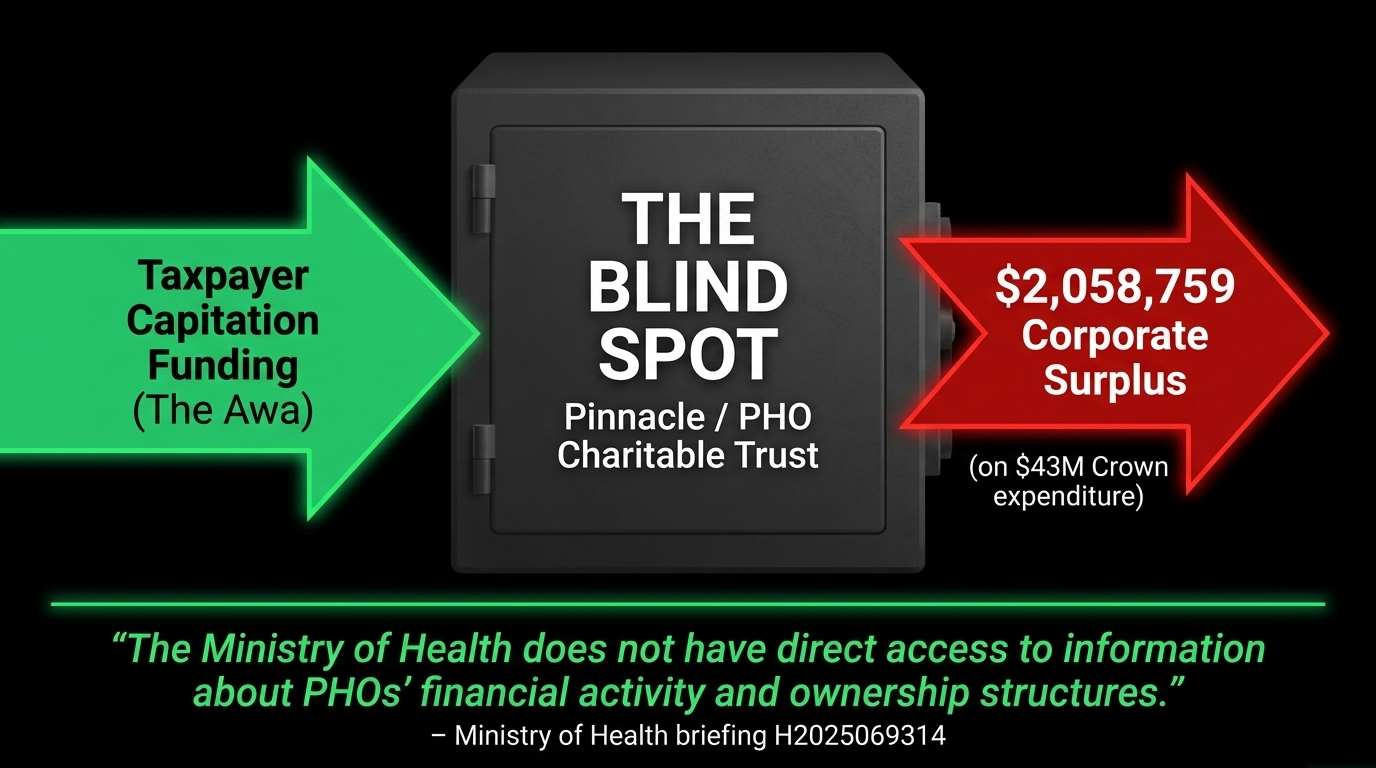
Six strands. One web. Completely closed. Completely self-reinforcing. Completely invisible to the Ministry that funds it — because as Ministry of Health briefing H2025069314 admits with breathtaking candour:
"The Ministry of Health does not have direct access to information about PHOs' financial activity and ownership structures."
The Crown is funding a machine it cannot see inside. And the man who helped build the machine is now advising the Minister who controls the funding.
That is not a health system. That is a heist with a WONCA fellowship.
Ko Te Kura Rata — The Medical School Born From a Corrupt Bargain
The University of Waikato Medical School is the most politically contaminated education project this country has produced in a generation. The origin story is documented in forensic detail by Democracy Project's Bryce Edwards — and it reads like a case study in how neoliberal governments transfer public money to private networks:
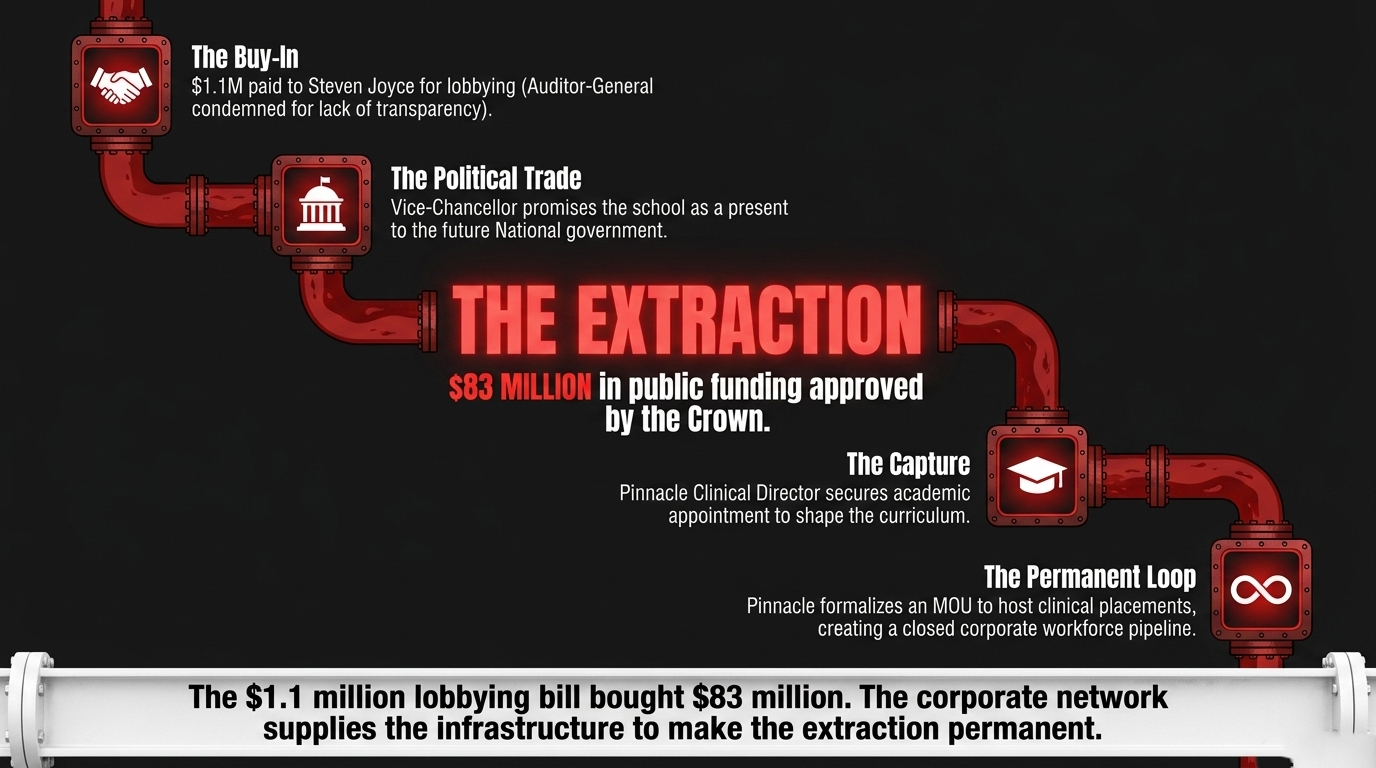
- Former National Finance Minister Steven Joyce was paid $1.1 million by Waikato University — without competitive tender — to lobby his former National colleagues for the school
- The Auditor-General published an open letter condemning the process as lacking transparency, and found Waikato "unwilling to account to the public"
- Vice-Chancellor Neil Quigley — simultaneously Chair of the Reserve Bank — was in personal contact with National health spokesperson Shane Reti and emailed him to say the school could be "a present" to a future National government
- The University advertised for a property developer before Cabinet had approved funding — because, as Edwards confirmed, they were confident in "the strength of its political connections"
- Despite Treasury, TEC, and the Ministry of Health all questioning whether a third school would actually improve rural doctor numbers, the Government approved $83 million in July 2025, confirmed by The Spinoff
And Scott-Jones?
He was publicly advocating for the school as Pinnacle Clinical Director during the lobbying campaign's peak intensity in July 2023 — on Pinnacle's own platform — declaring
"Pinnacle will collaborate with the incoming government, ensuring the implementation of policies that enhance education and training."
The incoming government he was anticipating was National. The policies that followed have directly benefited the corporate network he leads.
He then contributed to the business case justifying the funding. He then accepted the academic appointment from the institution that funding built. And in November 2024, Pinnacle formalised an MOU with the University of Waikato to host clinical placements across the Pinnacle network — meaning Pinnacle practices will train the graduates, Pinnacle ideology will shape their professional formation, and Pinnacle employment will be the natural destination of the workforce this school produces.
The $1.1 million lobbying bill bought $83 million in public funding. Scott-Jones supplied the clinical credibility that made it look like healthcare. Pinnacle will supply the infrastructure that makes it permanent.
As the Māori Green Lantern documented in Te Ara Utu: The Toll Road to Nowhere, this is the template this government applies in every portfolio: manufacture the policy rationale, embed the private beneficiary before the funding is announced, transfer the public asset, and call the extraction "investment."
Ko Wai a Simeon Brown? — The Minister Who Has No Business Being a Minister
Simeon Brown did not stumble into this appointment. He executed it deliberately, as part of a documented privatisation agenda that the Māori Green Lantern has tracked relentlessly across multiple investigations.
As documented in Exposing Simeon Brown's Dangerous Health Agenda:
- Brown's government cut 2,740 health sector jobs while declaring primary care a priority
- He disestablished Te Aka Whai Ora — the Māori Health Authority, the most significant structural advance for Māori health in a generation — confirmed by PMC peer review
- He proposed cuts to 246 roles specifically supporting Māori and Pacific health services, including the entire Māori health team within the National Public Health Service
- He imposed a $660 million savings target on Health NZ while simultaneously outsourcing 8,631 elective procedures to private hospitals, as documented in The Manufactured Crisis
- He is pursuing sweeping health legislation changes that dismantle the remaining equity architecture in the health system
The Listener described his model plainly:
"patient-centred" means "more outsourcing to the private sector."
The Public Service Association has confirmed this is the classic neoliberal playbook:
"deliberately underfund public services, then claim privatisation as the only solution."
And into this machine, Brown placed Dr Jo Scott-Jones
— the Clinical Director of the corporate network that stands to profit most directly from every policy the PCAG recommends.
In E Rua Ngā Rangi, the Māori Green Lantern documented how Brown's model devolves power to Pākehā corporate networks while centralising control over Māori health decision-making. This PCAG appointment is that dynamic made flesh: a Pākehā corporate GP given ministerial advisory power over the primary care system that his company dominates, while Māori health providers — underfunded, understaffed, structurally excluded — watch from outside the room.
This is not governance. This is a carve-up. And it is happening in public, in broad daylight, with a press release and a Distinguished Fellowship.
Ngā Pae o te Hauora Māori — The Outcome Catastrophe That Indicts Every Strand of the Web
Now the data. Because this is where the web kills people.
The Te Tauraki Independent Māori Statutory Board's 2025 Monitoring Report — covering the Eastern Bay of Plenty, the very takiwā where Scott-Jones has operated for three decades — confirms that Māori across the region experience persistently, catastrophically worse health outcomes than non-Māori across every major indicator: cancer, cardiovascular disease, diabetes, mental health, and access to primary care. Not marginally worse. Dramatically, measurably, preventably worse. After thirty years of the PHO model. After thirty years of Pinnacle. After thirty years of public money flowing through this architecture.
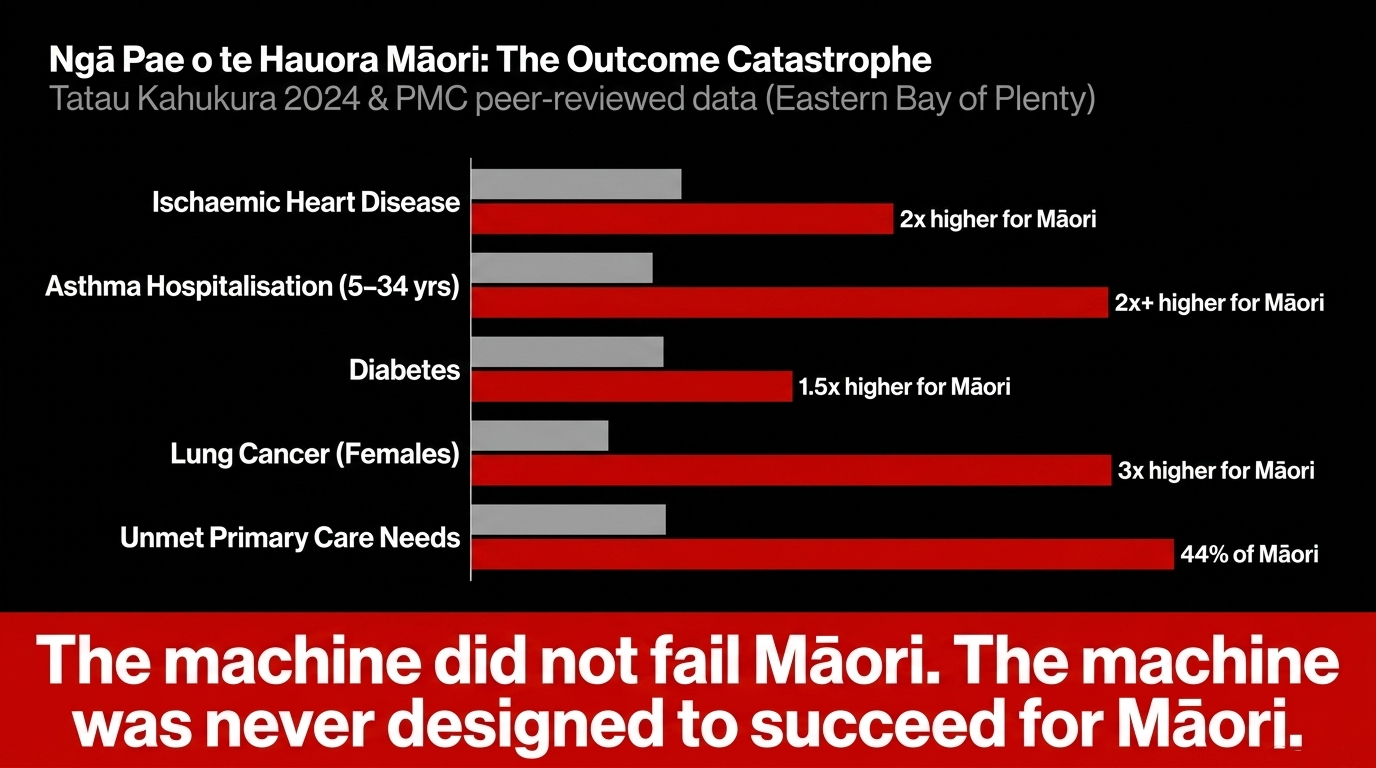
The Ministry of Health's Tatau Kahukura 2024 puts national numbers to the local catastrophe:
- Māori ischaemic heart disease rates twice those of non-Māori
- Māori females with lung cancer registered at over three times the non-Māori rate
- Māori 1.5 times more likely to have diabetes
- Māori aged 5–34 years more than twice as likely to be hospitalised for asthma
A peer-reviewed PMC/NZMJ study published in 2024 found 44% of Māori have unmet primary care needs — thirty years after the system claiming to serve them was built. And a BMC Health Services systematic review concluded plainly that "despite three decades of policy initiatives to improve integration of health care, delivery of health care in New Zealand remains fragmented, and health inequities persist for Māori."
The NZ Herald confirmed that Māori were systematically undercounted and under-resourced in health funding calculations from the beginning — meaning the PHO capitation model was structurally biased against Māori providers before the first dollar was ever paid.
The machine did not fail Māori. The machine was never designed to succeed for Māori. And the people who built and maintained the machine have been given awards and professorships and ministerial advisory appointments for their trouble.
Toru Tauira — Three Examples of Quantified Harm and Their Tikanga Violation
Example One: The Capitation River Diverted
In Western terms: you pay taxes to fund universal healthcare. Your taxes flow to a PHO. The PHO flows to a charitable trust. Above the charitable trust sits a private corporate membership body — Pinnacle Incorporated — that controls the technology, training, and practice infrastructure the trust depends on. Pinnacle's 2019-20 annual report recorded a surplus of $2,058,759 on $43 million of Crown-sourced expenditure, as confirmed in Pinnacle's own Annual Report.
The Ministry of Health admits it cannot see the financial flows.
You are funding a machine whose internal architecture is invisible to the government that funds it.
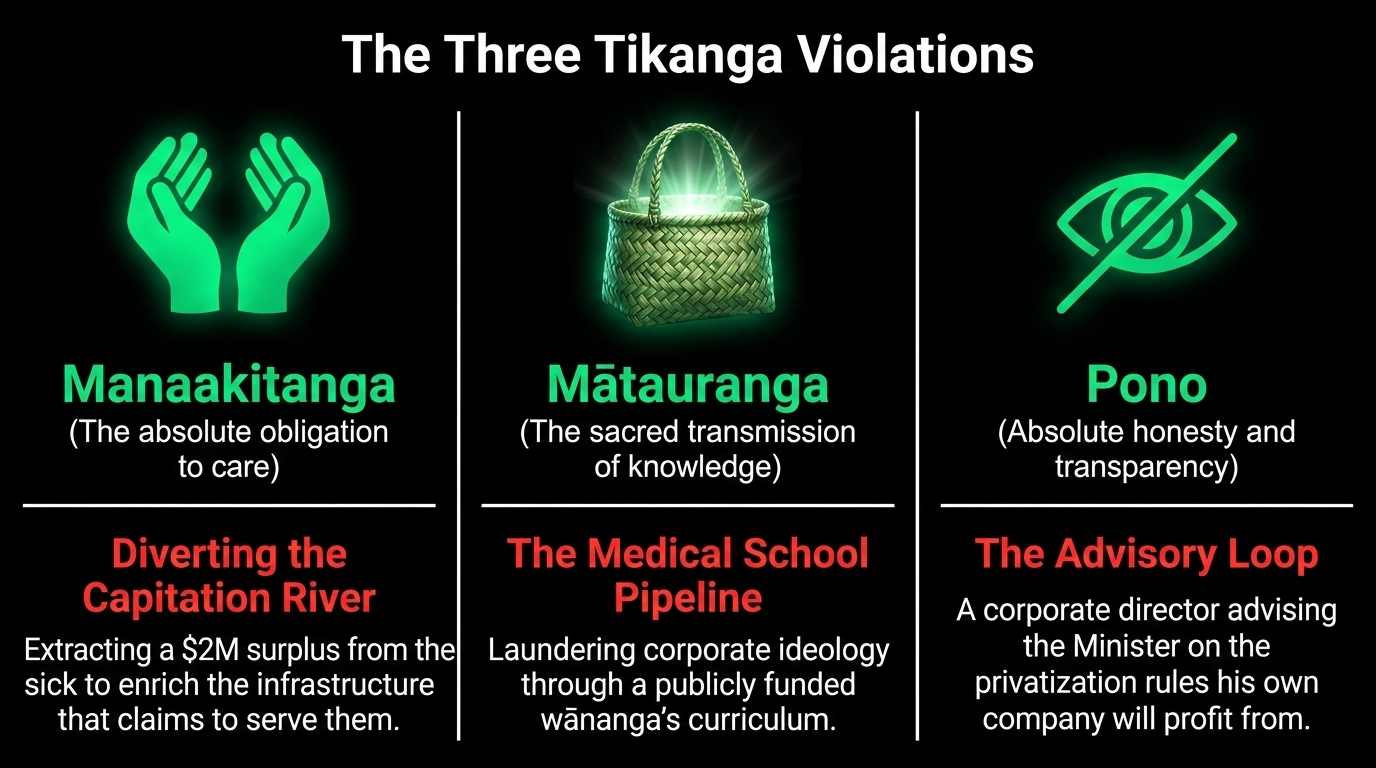
The tikanga violation is the desecration of manaakitanga — the absolute, unconditional obligation to care for those in your whare with everything you have. A system that extracts surplus from the sick to enrich the infrastructure that claims to serve them has not merely failed manaakitanga. It has weaponised manaakitanga's language to conceal its opposite.
Example Two: The Medical School Pipeline — Ideology Laundered Through Curriculum
In Western terms: imagine that Goldman Sachs funded a law school, Goldman Sachs partners taught the curriculum, Goldman Sachs offices hosted the clinical placements, and Goldman Sachs employment was the presumed career pathway for graduates — all funded by public money.
You would immediately recognise that as regulatory capture of the legal profession at its formation. That is precisely what is happening with the Waikato Medical School and Pinnacle.
The University of Waikato MOU formalises Pinnacle as a clinical placement partner. Scott-Jones — Pinnacle's Clinical Director — holds the academic appointment shaping the curriculum. The business case justifying $83M in Crown funding lists him as a named contributor. The graduates of this school will be professionally formed inside Pinnacle's ideological and commercial framework — and they will believe it is medicine, because it is all they will have seen.
The tikanga violation is the desecration of mātauranga — the sacred transmission of knowledge from those who hold it to those who will carry it forward. When the wānanga is captured by the interests of those who fund it, it no longer transmits knowledge. It transmits the ideology of those who own the infrastructure. As documented in The Nursery of Cages, this government specialises in building institutions that reproduce inequality while calling it education.
Example Three: The Advisory Loop — The Fox Inherits the Henhouse
In Western terms: a pharmaceutical company executive sits on the government committee that sets pharmaceutical pricing.
A construction company owner sits on the committee that awards public building contracts. A private GP corporate director sits on the committee that sets the funding rules and privatisation pathway for primary care. Each of these is an obvious, disqualifying conflict of interest.
Only the last one happened, confirmed by the Beehive on November 2, 2025. Scott-Jones's corporate network stands to directly profit from every recommendation the PCAG makes about "shifting hospital care into the community." He is, in the most literal sense, writing the policy his company will implement, for the Minister who benefits politically from the privatisation it enables.
The tikanga violation is the desecration of pono — the absolute requirement of honesty and transparency in all things. Pono is not just personal integrity. It is the structural condition for trust between people, between communities, and between those who hold power and those over whom it is exercised. When the person advising on the rules is the person who profits from them, pono has been destroyed at the root. The whare cannot stand when its foundations are deception.
As the Māori Green Lantern examined in Neoliberal Vultures Circle as Health NZ Bleeds, this is the consistent pattern: manufacture the crisis, place the beneficiary in the advisory role, implement the policy, call the extraction "reform."
Ko te Aho Matua — The Pattern Named, The Whakapapa of Harm
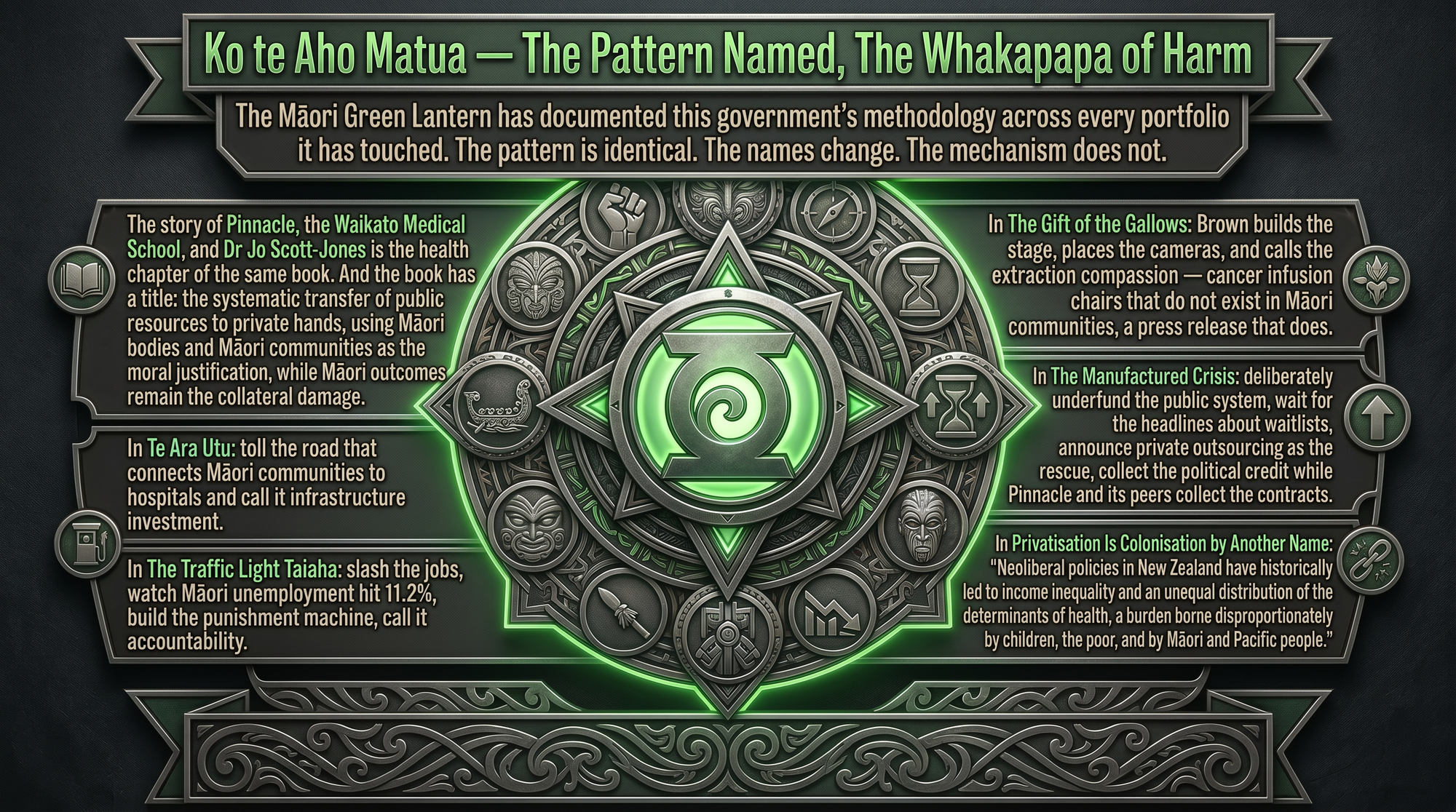
The Māori Green Lantern has documented this government's methodology across every portfolio it has touched. The pattern is identical. The names change. The mechanism does not.
In The Gift of the Gallows: Brown builds the stage, places the cameras, and calls the extraction compassion — cancer infusion chairs that do not exist in Māori communities, a press release that does.
In The Manufactured Crisis: deliberately underfund the public system, wait for the headlines about waitlists, announce private outsourcing as the rescue, collect the political credit while Pinnacle and its peers collect the contracts.
In Privatisation Is Colonisation by Another Name: "Neoliberal policies in New Zealand have historically led to income inequality and an unequal distribution of the determinants of health, a burden borne disproportionately by children, the poor, and by Māori and Pacific people."
In The Traffic Light Taiaha: slash the jobs, watch Māori unemployment hit 11.2%, build the punishment machine, call it accountability.
In Te Ara Utu: toll the road that connects Māori communities to hospitals and call it infrastructure investment.
The story of Pinnacle, the Waikato Medical School, and Dr Jo Scott-Jones is the health chapter of the same book. And the book has a title: the systematic transfer of public resources to private hands, using Māori bodies and Māori communities as the moral justification, while Māori outcomes remain the collateral damage.
Te Ara Whakamua — What Accountability Now Demands
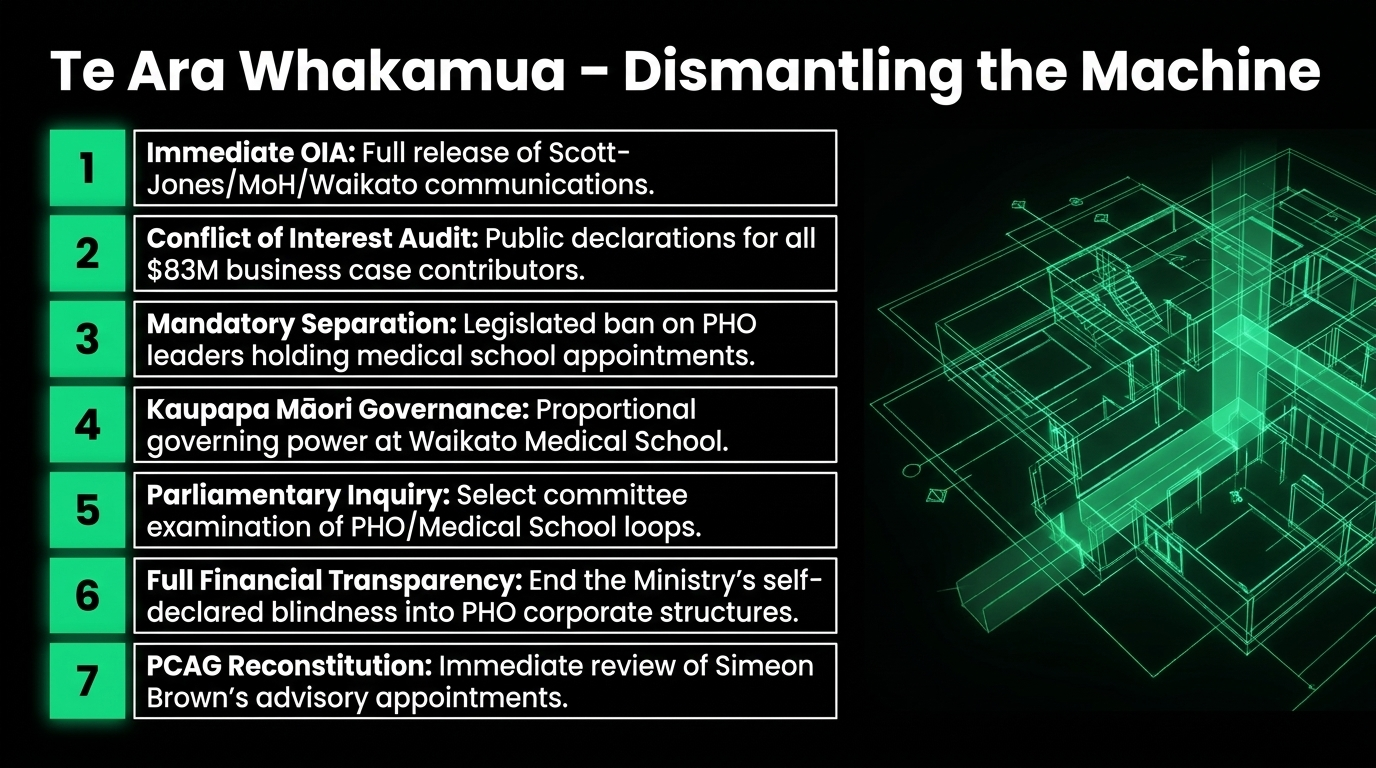
The solutions are clear. They are resisted only because they threaten the machine:
Immediate OIA — full release of all communications between Scott-Jones, Pinnacle, Waikato University, and Ministry of Health officials regarding the medical school business case. File it today at FYI.org.nz
Conflict of Interest Audit — all named contributors to the MoH New Medical School Business Case must publicly declare all commercial relationships with entities that benefit from the school's operation
Mandatory Separation — legislated prohibition on corporate PHO leadership holding academic appointments at publicly funded medical schools whose clinical placement networks include that corporation's practices
Kaupapa Māori Governance — proportional Māori governance (not advisory, not consultative — governing) at the Waikato Medical School, reflecting the Māori population of the Midlands region
Parliamentary Inquiry — select committee examination of the circular conflict of interest between PHO corporate networks and the publicly funded medical school designed to supply their workforce
Full Financial Transparency — legislated visibility for all PHO-linked corporate structures, including parent companies, technology arms, and venture subsidiaries — ending the Ministry's self-declared blindness forever
PCAG Reconstitution — immediate review of all PCAG appointments for undisclosed conflicts of interest; Scott-Jones's position is the most obvious starting point
The taniwha does not leave the awa voluntarily. You redirect it — with legislation, with transparency, with the power of whānau who refuse to be silent.
Kia tū tonu tātou. The web is named. The taniwha is named. The machine is named. Now we dismantle it.
Kia kaha. Kia māia. Kia manawanui.
The Māori Green Lantern — Ivor Jones
17 April 2026
He Koha Whakaaro — Why This Mahi Costs and Why Whānau Must Fund It
The taniwha spun his web across thirty years and $83 million of public money. He collected the capitation. He built the corporate network. He wrote the government's funding application for the school that will train the next generation inside his ideology. He accepted the ministerial appointment. He received the international award.
And nobody put it all in one place until now.
This essay did what the Ministry of Health admitted it cannot do — it traced the financial and institutional architecture of a closed conflict of interest loop at the heart of New Zealand's primary care privatisation project. It took tools, time, research skills, and the absolute refusal to be intimidated by the power of the people it names.
The Crown will not fund this. Pinnacle certainly will not fund it. Simeon Brown has proven he funds the people who benefit from the machine, not the people who expose it.
Whānau fund this. And this essay is the proof of what that funding produces.
Every koha says:
we see the taniwha, we name it, we map its channels, and we refuse to let it drain our awa in silence.
Three pathways, whānau:
Direct support for this mahi: Koha — The Māori Green Lantern
Essays like this one direct to your inbox: Subscribe at themaorigreenlantern.maori.nz
Direct bank transfer: HTDM, account number 03-1546-0415173-000
Facebook: Follow and subscribe here
If koha is not possible right now — no worries, not even a little. Share this essay. Send it to your whānau in the Eastern Bay. Send it to your local MP. Post it in your community group. Send it to every health journalist in this country. That kōrero is rangatiratanga. That truth-spreading is the taiaha in the hands of the people.
Kia kaha, whānau. Stay vigilant. Stay connected. The awa belongs to the people.

Research conducted April 15–17, 2026. Sources verified: Ministry of Health New Medical School Detailed Business Case (proactively released), Ministry of Health PHO Finances Briefing H2025069314 (proactively released), Ministry of Health MOU with University of Waikato, Beehive.govt.nz, The Spinoff, NZ Herald, Democracy Project/Bryce Edwards, Auditor-General public statements, Pinnacle annual reports, Pinnacle news releases, University of Waikato LinkedIn, Church Street Surgery Ōpōtiki, LinkedIn public profile, Te Tauraki IMPB Monitoring Report 2025, Tatau Kahukura Māori Health Chart Book 2024, Waitangi Tribunal Wai 2575 data, BMC Health Services Research peer review, PMC peer reviews 10354830 and 10898093, Hapai Te Hauora, The Māori Green Lantern archive. All URLs live-tested at time of publication.