"THE GIFT OF THE GALLOWS: Simeon Brown's Cancer Infusion Con and the Architecture of Māori Death" - 13 April 2026
They gave you 14 chairs and sold you the medicine. They built the stage, hired the cameras, and called it compassion. We call it colonialism with a drip bag.

Tēnā koutou katoa.
Picture a gravedigger who shows up to your marae with a brand new shovel. He presents it to the whānau — gleaming, sharpened, modern — and announces he has "expanded access to burial services." He smiles for the camera. The Breast Cancer Foundation cautiously praises the quality of the shovel. RNZ runs the press release. Nobody asks who commissioned the grave.
This is Simeon Brown's cancer infusion announcement.
The Deep Dive Podcast
Listen to a lively conversation between two hosts, unpacking and connecting topics in the sources of this essay.

On Monday, the Health Minister stood at Waitākere Hospital and told New Zealanders he was delivering 14 new infusion centres and expansions at 14 existing sites — "hundreds" more cancer treatments a week, "thousands" more patients, "life-saving treatment closer to home," as RNZ reported. It sounds magnificent. It is a conjuring trick. And the hand that isn't being watched is the one routing publicly-funded cancer medicine into private profit, stripping Te Tiriti from health legislation, and locking in 10-year privatisation contracts that no future government will reverse without a political war.
He built you a chair. Then he sold the medicine.
The Historical Whakapapa of This Theft

This government did not invent this playbook. It inherited it, refined it, and weaponised it.
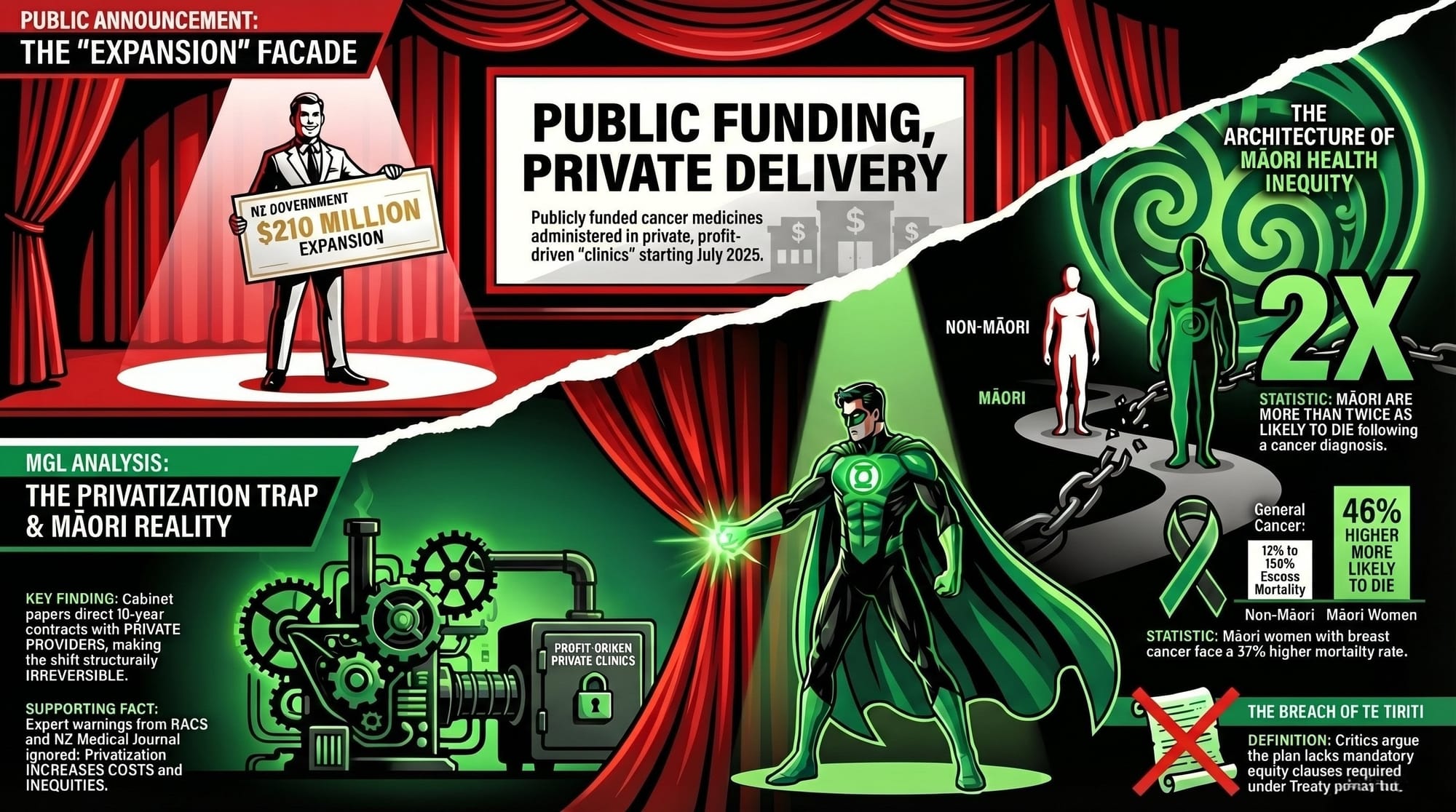
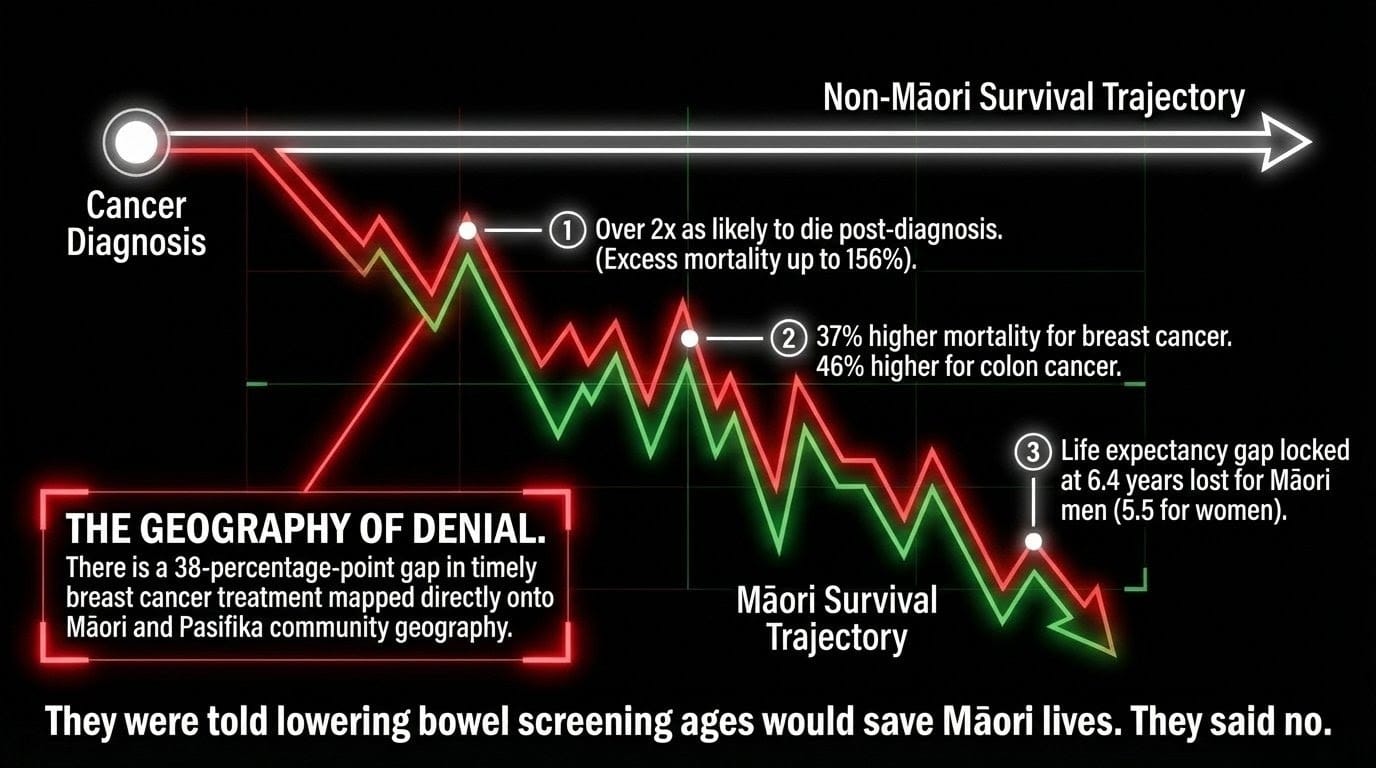
As Te Ara's history of Māori health confirms, Māori men were almost three times more likely to die of lung cancer than non-Māori men, and Māori women were over four times more likely. A peer-reviewed study in the Journal of Clinical Oncology found Māori were more than twice as likely to die after a cancer diagnosis as non-Māori, with excess mortality ranging from 12% to 156% across cancer types. Māori women with breast cancer are 37% more likely to die than non-Māori women. Māori with colon cancer are 46% more likely to die.
The ASMS Toi Mata Hauora report Māori health, Te Tiriti o Waitangi, and the impacts of outsourcing — commissioned by New Zealand's own salaried medical specialists — is unambiguous: in 2025, the life expectancy gap between Māori and the population remains 6.4 years for men and 5.5 years for women. Māori experience worse survival rates for 23 out of 24 of the most common cancers in Aotearoa. The Crown has acknowledged this. The Waitangi Tribunal has ruled on it. And now the Crown is outsourcing cancer treatment to private providers with no legal obligation to fix it.
The Announcement — The Con in Full
Here is what Brown told you: a $210 million investment from Budget 2024 is funding new public infusion centres, 66 new Pharmac medicines including 33 cancer treatments, and 218 more chair-days per week. Every sentence is technically true. Every sentence is a distraction.
Here is what Brown did not tell you: from 1 July 2025, those same publicly-funded cancer medicines began being administered in private hospitals and clinics. When challenged, Pharmac's own consultation document confirmed in plain language: "Please note that this consultation is not proposing a change in Government policy — a decision on that matter has already been made by the Government."
Pharmac didn't decide this. Brown and Seymour decided this. Pharmac was handed a fait accompli and told to rubber-stamp it. As the Beehive's own press release confirms, by December 2025 the first cancer medicine was available in private clinics. The medicine was publicly funded. The clinic is privately owned. The profit goes nowhere near your whānau.
The Smoking Gun: Read the Man's Own Words
Do not trust the press release. Read the cabinet paper.
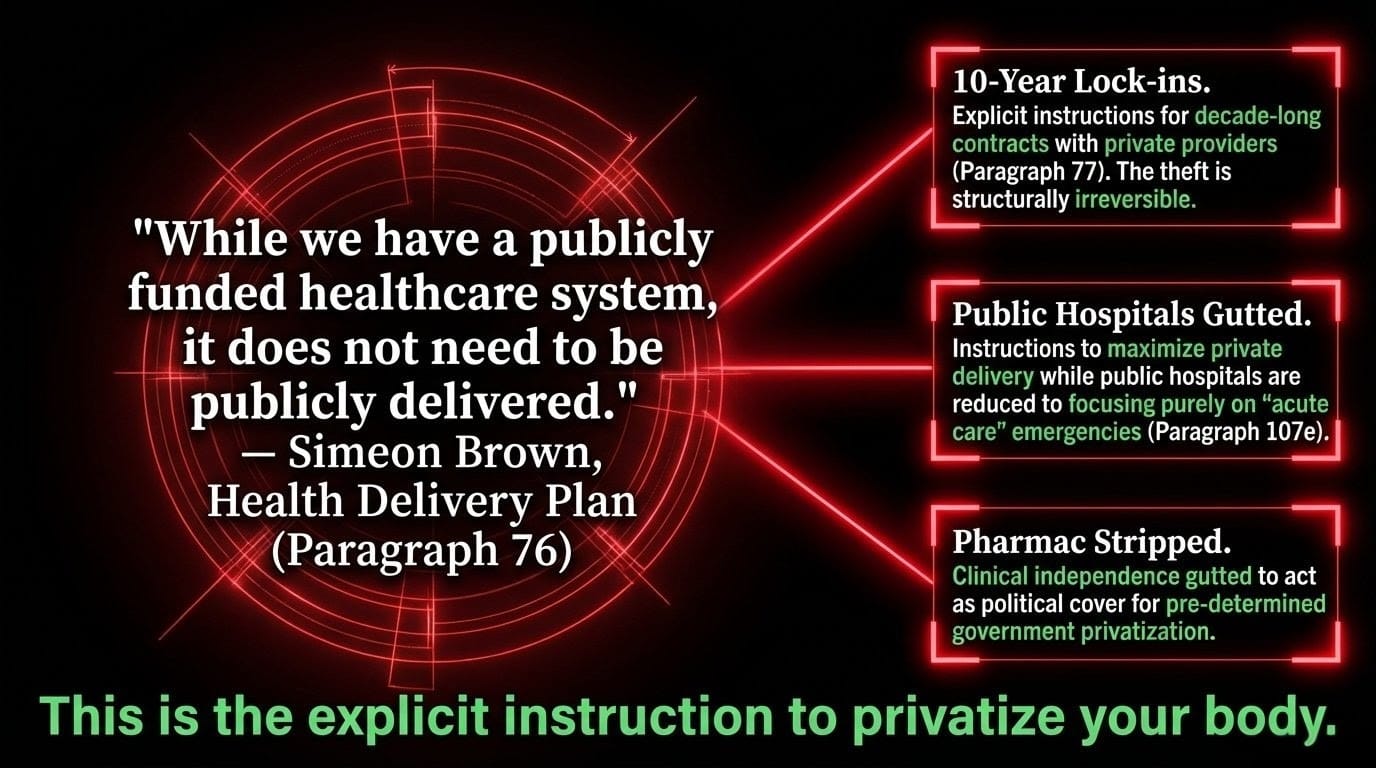
In Brown's Health Delivery Plan he writes at paragraph 76:
"While we have a publicly funded healthcare system, it does not need to be publicly delivered."
There it is. Fourteen words. The entire architecture of this government's health policy. Public money. Private delivery. Your taxes build the clinic. A shareholder takes the dividend.
Brown then instructs Health NZ in the same document that his expectations for private sector outsourcing "will extend to many other patient services such as radiology and cancer treatments" (paragraph 78), directs 10-year contracts with private providers (paragraph 77), calls for Public Private Partnerships (paragraph 107j), and instructs that public hospitals should "focus on acute care" by maximising private delivery (paragraph 107e). Translated from bureaucrat: strip the public hospitals down to emergencies. Hand everything else — including your cancer infusion — to the private sector. Lock it in for a decade. Call it "innovation." Call it "life-saving treatment closer to home."
It is the privatisation of your body. The minister wrote the instructions himself.
Five Hidden Connections — All Verified, All Devastating

Connection One: The $604 Million Pharmac Boost Was a Private Sector Feeding Trough. Those 66 new funded medicines create immediate infusion demand that private clinics are now authorised to capture through Health NZ's transitional access framework. The government manufactures the demand with public money. The private sector drinks from the trough. Your cancer is a product line.
Connection Two: Pharmac Was Ordered — It Did Not Choose. Pharmac's own consultation document confirmed the government's decision was made before any consultation began. Pharmac's clinical independence — hard-won over decades — was gutted and used as political cover. That is institutional corruption.
Connection Three: The Elective Surgery Model Is the Blueprint for Your Death. This government has already outsourced 22,175 elective procedures to private providers in 2024/25, as a Health NZ OIA response confirms. The ASMS report is explicit: outsourcing "works especially well for those who are more well off, and for 'white' populations" while having "the very real potential to increase inequities for Māori." The Auditor-General has already confirmed Elective Boost does not equitably benefit all populations. The evidence is in. The government continues.
Connection Four: Health NZ Governance Has Privatisation Interests Baked In. As The Māori Green Lantern previously investigated in The Charity of Conquerors, this government has made a pattern of socialising the cost of public services while privatising the return. The fox is not in the henhouse. The fox is chairing the henhouse board and drafting the henhouse policy.
Connection Five: They Were Told the Policy Would Cost Māori Lives and Said No Anyway. As the NZ Herald reported in March 2025, health officials advised the government that significantly more Māori and Pasifika lives would be saved by lowering bowel cancer screening ages further for those populations. Ministers rejected this advice. This is not negligence. It is racialised policy-making dressed in the language of neutrality.
Three Examples for the Western Mind
Example One: England — They Counted the Bodies
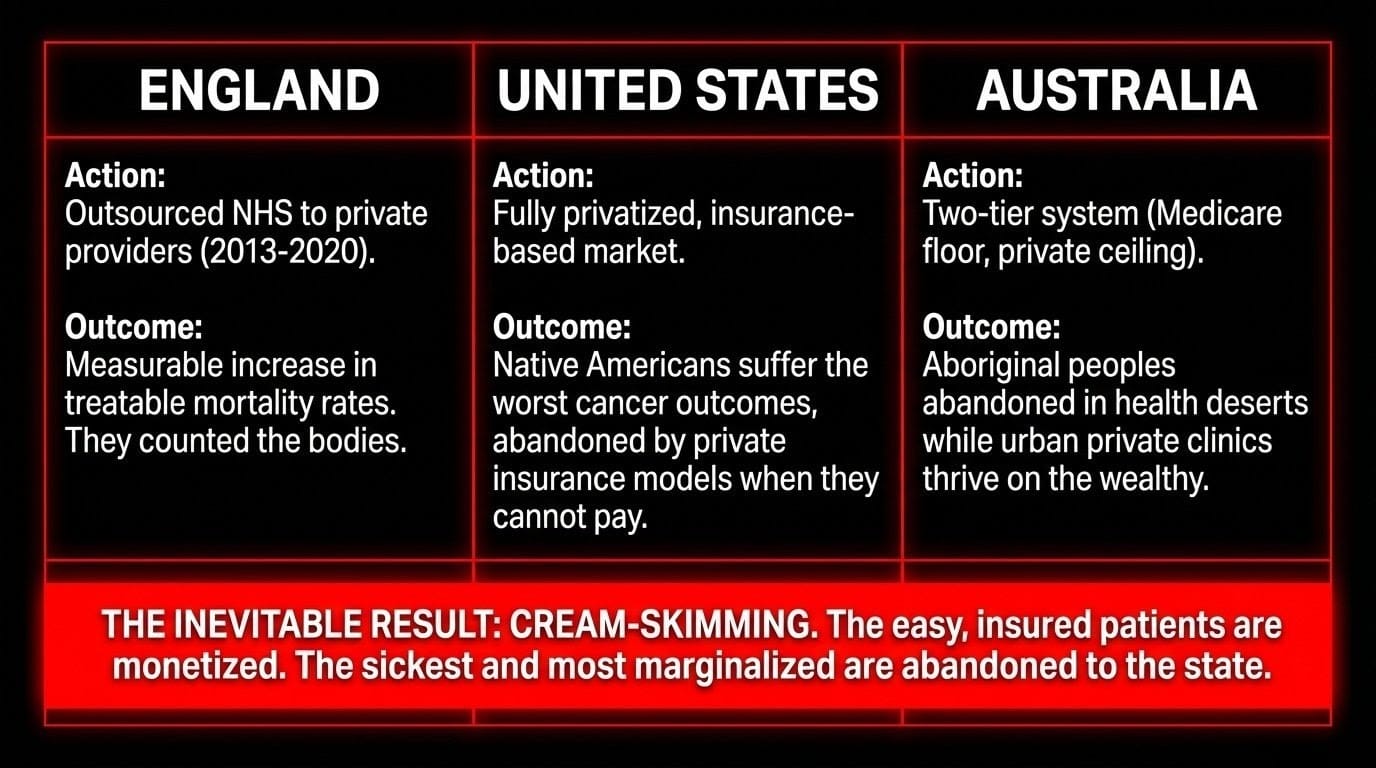
Between 2013 and 2020, Conservative governments progressively outsourced NHS services to private providers. Research cited directly by the ASMS Toi Mata Hauora report found a measurable increase in treatable mortality rates — people who died of conditions that should have been successfully treated. Not a modelled risk. They counted the bodies. England tried what Brown is building. Brown has read this evidence. He knows.
What this means for tikanga: Imagine your grandmother gets cancer. She can see the new infusion clinic from her window — but it only takes patients with Southern Cross insurance. She waits six months in the public queue while the private clinic runs at 70% capacity. That is not access. That is theatre. In tikanga terms, this violates manaakitanga — the sacred duty of unconditional care that does not discriminate by wealth. When the state converts health into a market, it turns a wāhi ora into a wāhi tauhokohoko — a place of transaction — destroying the mauri of the system itself.
The solution: Direct the $210 million into Health NZ workforce capacity. Require all publicly-funded cancer medicines to be administered in public facilities as the default. Mandate binding Te Tiriti compliance as a condition of every private provider contract, as the ASMS report recommends.
Example Two: The United States — The Complete Catastrophe
The United States built the world's most comprehensively privatised healthcare system. It spends more per capita on health than any comparable nation. Native Americans — Indigenous peoples with a colonial dispossession history directly parallel to Māori — have among the worst cancer outcomes of any population group in the country. They are diagnosed later. They are treated less. They die sooner. The private insurance-based system abandons them when they cannot pay. This is not a failure of the American private health model. It is its logical outcome.
As the NZ Medical Journal warned in its analysis of Brown's plan, cream-skimming — where private providers take the easy, insured, less-complex patients — leaves the public system with the sickest, most marginalised patients and less funding to treat them. In Aotearoa, that population is disproportionately Māori.
What this means for tikanga: In te ao Māori, health is not individual — it is whakapapa. The death of a kuia from preventable cancer severs a link in the chain of mātauranga, aroha, and identity that sustains hapū and iwi across generations. Brown's delivery plan cannot measure that loss — which is exactly why it does not try.
The solution: Immediately audit the ethnic composition of patients accessing cancer treatment through private providers receiving public funding. Require all 10-year outsourcing contracts to include binding equity clauses with penalties for underrepresentation of Māori and Pasifika. Reinstate a Māori-led health governance body with statutory authority to veto privatisation decisions that breach Te Tiriti.
Example Three: Australia — The Aboriginal Mirror
Australia runs a two-tier health system with Medicare as the public floor and a dominant private sector above it. Aboriginal and Torres Strait Islander peoples have the worst cancer mortality rates in Australia — a gap that has resisted decades of promises precisely because private providers concentrate in affluent urban areas and abandon First Nations communities in remote regions. The pattern is identical to what Brown is engineering.
The ASMS report is explicit: outsourcing in Aotearoa is "always with non-Māori providers… meaning Māori patients and their whānau are unlikely to have the option to access outsourced services from Māori providers." And all available material on Elective Boost is, in the ASMS report's precise word, "silent" on the role of Māori in decision-making and investment. Meanwhile the Breast Cancer Foundation's own data — buried in Brown's press release — confirms a 38-percentage-point gap in timely treatment by location, mapped almost perfectly onto Māori and Pasifika community geography.
What this means for tikanga: Imagine a government declared all waka would now be privately operated — available for a fee. If you could not pay, you would wait for the state waka — eventually. They would call the new policy "Waka Access Expansion" and hold a press conference on the beach. That is this announcement. The waka is real. The tino rangatiratanga — self-determining access to care as a right, not a market outcome — is gone.
The solution: Mandate that any private provider receiving publicly-funded cancer medicine contracts must achieve Māori and Pasifika patient access rates proportional to population health need within 24 months or lose accreditation. Invest in Māori-owned health providers to expand into specialist cancer care. Implement all six equity recommendations from the ASMS Toi Mata Hauora report — not one of which this government has touched.
The Experts: Unanimous. Ignored.
The Royal Australasian College of Surgeons opens its position statement with one sentence: RACS does not support outsourcing to the private sector.
The NZ Medical Journal states Brown's plan
"is at serious risk of breaking it further, increasing health costs, decreasing productivity."
The Green Party states: funding the private sector "will cost more, create more strain on public providers, and deepen the already existing inequities."
The NZMJ's earlier PPP analysis confirmed Māori had 1.67 times the rate of major trauma hospitalisation compared to non-Māori — the exact complex patient population private providers will reject and public hospitals will be left to carry with less money.
RACS. NZMJ. Green Party. ASMS. Auditor-General. All saying the same thing. Brown nods. Seymour claps. The 10-year contracts are drafted in silence.
Previous MGL Analysis: The Pattern Has a Whakapapa

In The Pātaka is Ash, this analysis documented the core neoliberal circuit: announce public investment, route the benefit to those who already have, call the press conference "equity." The cancer infusion announcement runs the same circuit.
In The Charity of Conquerors, the tikanga violation was named precisely: the state socialises the cost and privatises the return. The hau of sacrifice is never returned. Brown's cancer announcement is this principle applied to oncology.
In The Pātaka Beside the Strait, the analysis exposed how this government weaponises the language of sovereignty — "patient choice," "access," "efficiency" — while advancing the structural opposite. Brown's phrase "closer to home" is exactly this: slogan sovereignty deployed to obscure structural extraction.
In The Nursery of Cages, the deeper logic was confirmed: this state does not accidentally harm Māori. It is structurally built to do so. The announcement of expansion without equity is not a planning gap. It is the plan.
The Tikanga Verdict
Brown's Health Delivery Plan states care will be prioritised "based on clinical priority, not race" (paragraph 107a). This sentence is not neutral. It is a weapon. It erases systemic racism as a determinant of clinical outcome. It pretends Māori arrive at the infusion chair from the same starting line as a Pākehā professional in Remuera with private insurance. It treats centuries of dispossession, racially biased clinical triage, and geographic health deserts as irrelevant to "clinical priority."
The ASMS Toi Mata Hauora report is explicit: the Waitangi Tribunal's five principles — active protection, equity, options, partnership, and tino rangatiratanga — are not visible anywhere in this government's cancer infusion framework. Not inadequately reflected. Not visible at all.
This is not a policy failure. It is a Treaty breach. It is ongoing colonisation administered through a budget spreadsheet, announced at a press conference with scissors and a smile.
The Logic of the Lie — Named, Numbered, Destroyed

- The government is routing publicly-funded medicines to private clinics — as Pharmac confirmed was a political decision made before any consultation.
- Brown's own cabinet paper declares publicly-funded healthcare "does not need to be publicly delivered."
- Health NZ is being directed to sign 10-year private contracts — as Brown's Health Delivery Plan explicitly states — making this structurally irreversible.
- RACS, the NZMJ, the ASMS, and the Green Party all confirm this worsens outcomes for Māori and Pasifika.
- The Breast Cancer Foundation's own data confirms a 38-percentage-point gap in timely treatment mapped directly onto Māori geography.
Brown is not building a stronger public cancer care system. He is building the infrastructure of its replacement, using your taxes as the foundation, your cancer as the commodity, and your whānau as the externality.
Rangatiratanga Demands We Name It
Ka whawhai tonu mātou.
Every data point in this essay was sourced from peer-reviewed research, government documents, medical specialist organisations, and the minister's own cabinet papers. Brown wrote it down. Seymour celebrated it publicly. Pharmac confirmed the political override. The Auditor-General confirmed the inequity. The NZMJ called it a breaking of the system. RACS rejected it outright.
What we are watching is a white supremacist neoliberal government do what such governments have always done: convert collective public goods into private profit streams, use the language of equity to deliver its opposite, and ensure that when the harm accumulates, it accumulates in the bodies of Māori, Pasifika, and the poor.
We name it. We document it. We will not stop.
Tino rangatiratanga does not ask permission to tell the truth.
The Koha Consideration
Whānau, Simeon Brown has a ministerial office and a government budget to spin a story about cancer chairs and compassion. What we have is this: the taiaha, the research, the cabinet papers they hoped you would never read, and you.
Every koha is a direct counter-strike against this architecture of Māori death being constructed in your name. If this essay prevented one whānau from being deceived — if it helped one rangatahi understand why their koro died waiting while the private clinic 20km away ran at 70% capacity using publicly-funded medicine — then every hour of this mahi was worth it.
Three pathways exist:
For those who wish to support this mahi directly:
Koha — Support the Māori Green Lantern
For those who wish to receive essays and support through subscription:
Subscribe to The Māori Green Lantern
For those who prefer direct bank transfer: HTDM | 03-1546-0415173-000
If you cannot koha — no worries, no shame. Subscribe, follow, and share this essay. That is koha in itself. Follow and read at themaorigreenlantern.maori.nz — share so this truth travels faster than the press release that tried to bury it.
Nō reira, tēnā koutou, tēnā koutou, tēnā koutou katoa.
Research conducted April 2026. Sources: RNZ | Pharmac | Beehive | Health NZ OIA | Brown's Health Delivery Plan | ASMS Toi Mata Hauora | NZ Medical Journal | RACS | Green Party | JCO — Māori cancer survival | Te Ara | NZ Herald | NZMJ PPP Analysis