"THE WAITING ROOM IS A GRAVE: How a White Supremacist Neoliberal Government Starved Primary Care, Sold the Body to Corporates, and Called It Health Reform" - 7 May 2026
They defunded your doctor, handed your hospital to three private companies, installed a commissioner who "cooked the books," dismantled the Māori Health Authority — and Māori whānau are paying with their lives.


🌟 E NGA WHĀNAU — THIS IS ESSAY NUMBER 1000 🌟

Tēnā koutou katoa.
Before you read a single word of what follows, pause.
This essay
— this taiaha raised in the digital age
— marks the 1000th piece published on The Māori Green Lantern.
One thousand essays. One thousand acts of resistance. One thousand times we chose rangatiratanga over silence.
When this platform began, it was a voice in the dark — one person, one keyboard, one refusal to accept that Māori would continue to be lied to without someone naming the liar.
What began as a whisper has become a roar.
In the months ahead, as the November 2026 election approaches, this voice will grow louder still.
By the end of 2026, this platform projects to reach 50,000 engaged readers across Aotearoa
— whānau, hapū, tauiwi allies, workers, students, and every person who believes that truth is the most dangerous thing a colonised people can wield.
The whakapapa of this initiative is simple: every essay is a thread in a kākahu that wraps whānau in the warmth of verified, unflinching truth. One thousand threads. Enough, now, for a cloak. Tēnā koe ki ēnei mahi.
Now read.
This essay examines the collapse of New Zealand's GP system, the systematic privatisation of public healthcare under the Luxon coalition government, and its disproportionate impact on Māori whānau
— because it directly affects access to primary healthcare.
This is a matter of public interest, Te Tiriti o Waitangi compliance, and democratic accountability of named public officials acting in their public capacity. This analysis activates the responsible communication defence under Durie v Gardiner NZCA 278 and qualified privilege under Lange v Atkinson 3 NZLR 385.
The Whakapapa of This Platform: 1000 Essays, One Refusal
The Māori Green Lantern did not begin with a business plan. It began with anger
— the kind that comes from watching your people be lied to, repeatedly, by people in suits who have never known what it is to choose between a GP visit and kai on the table.
One thousand essays later, the anger has not dimmed. It has been sharpened into evidence.
The Deep Dive Podcast
Listen to a lively conversation between two hosts, unpacking and connecting topics in the sources of this essay.
From the dismantling of Te Aka Whai Ora, to the privatisation of hospitals, to the exposure of the capitation funding con, to the naming of every minister and corporate player profiting from Māori ill-health — this platform has been the paper trail that power hoped would never exist.
By the end of 2026, on the eve of the most consequential election in a generation, this platform is projected to reach 50,000 readers. That is 50,000 people who will vote knowing what the mainstream media will not tell them. That is rangatiratanga in action.

Essay 1000 is not a celebration. It is a reckoning.
A Healing House Set on Fire, Then Sold to the Arsonist

Picture a whare hauora — a healing house — built on ancestral land.
For generations, people came here with their pain: the kuia whose joints ache in winter, the tamariki with asthma rattling through their chests at 3am, the rangatahi whose diabetes was never caught early enough.
The healers inside were underpaid, overworked, and exhausted — but they came anyway, because that is what tohunga do.
Now picture a government that cuts the wood supply for the fire. Slowly at first — 21% funding growth while costs rise 30%. They commission a report recommending 10–20% more firewood. They offer 4–5%. They burn the Māori wing down entirely — disestablishing the Māori Health Authority — and tell everyone it was done for
"efficiency."
Then they appoint a commissioner whose specialty is financial turnarounds, not healthcare.
He
"cooks the books."
He teaches two days a week at university while supposedly running the country's largest health bureaucracy. He oversees 2,000 job cuts. And when the public system is sufficiently broken, when the waitlists are long enough and the whānau desperate enough
— three private companies are handed 10-year contracts to pick up the patients the government starved out of the public system.
Then the government looks at the embers and calls it
"record investment in health delivery."
This is not metaphor. This is the verified, documented, source-cited truth of what Christopher Luxon, Simeon Brown, Lester Levy, and their corporate beneficiaries have done to your healthcare system. And Māori whānau are the ones dying outside in the cold.
The Numbers Are Damning
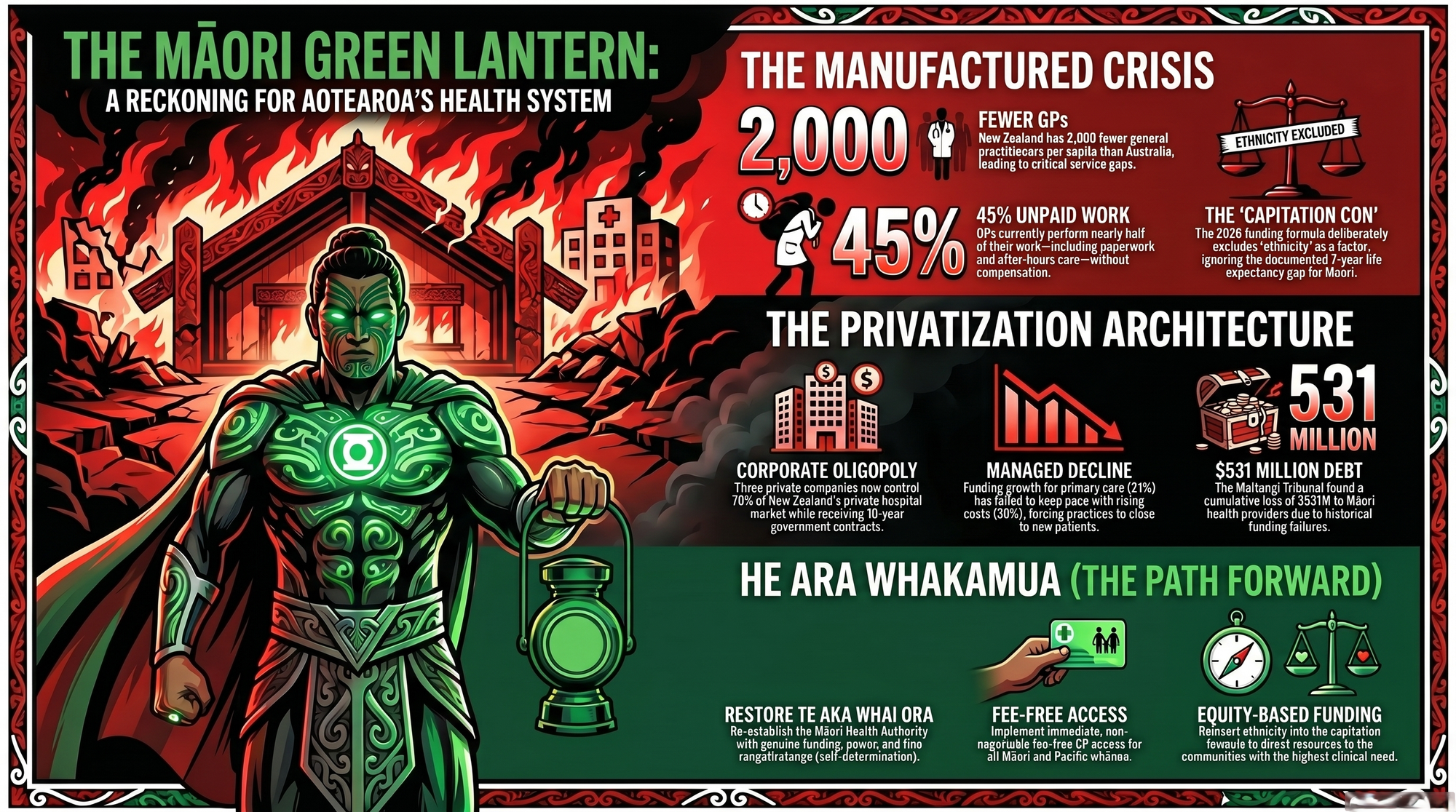
New Zealand has 2,000 fewer GPs per capita than Australia, as reported by RNZ.
Half of all New Zealand GPs report burnout — the highest rate of any country surveyed by the Commonwealth Fund, per the RNZCGP.
One third of practices cannot take on new patients. GPs are not paid for 45% of the work they do — face-to-face contact is just 55% of a GP's working day — as The Epoch Times' coverage of the RNZCGP collapse report documents.
If all 425 GPs over retirement age walked out tomorrow, approximately 725,000 patients would have no doctor.
The GP-to-population ratio is projected to fall from 74 per 100,000 in 2021 to just 70 in 2031. Ten extra GPs per 100,000 equates to roughly 30 fewer deaths annually from cancer, respiratory disease, and cardiovascular illness.
This government is choosing that death count. Health NZ projects needing an additional 3,450 doctors and 4,100 nurses by 2033 if current trends continue, as The Manufactured Crisis essay on this platform has documented.
The Capitation Con: A Funding Model Designed to Fail Māori
The root mechanism is the capitation funding model — introduced in 2002, never meaningfully updated, based on age and sex data from the 1990s, and deliberately blind to ethnicity, deprivation, and actual Māori health need.
As GP NZ chairman Bryan Betty told Newstalk ZB, it
"focuses on age predominantly, and not deprivation, co-morbidity and the other factors that really impact on health."
From 2009 to 2022, the consumer price index rose ~30% while primary care funding increased only ~21%, as documented by The Epoch Times.
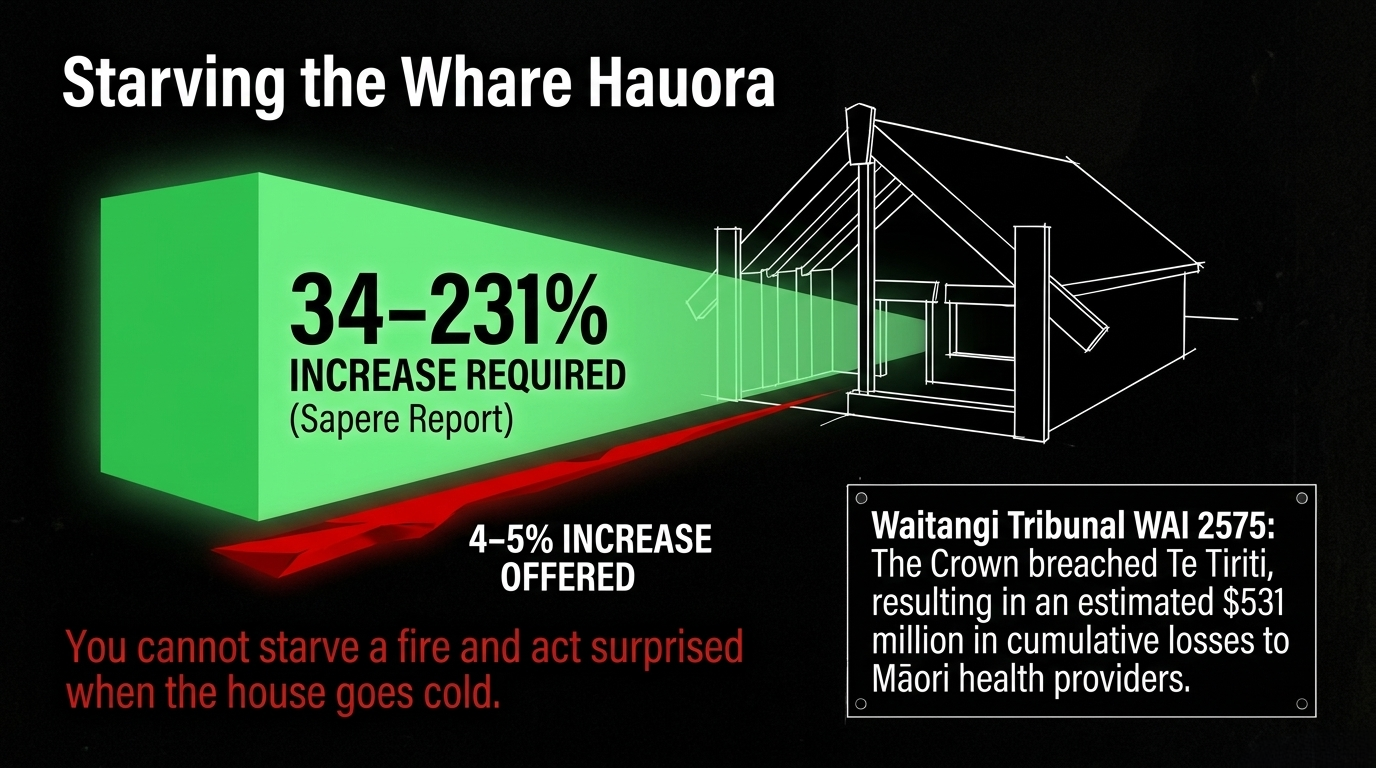
The government's own 2022 Sapere report recommended increases of 34–231% for high-needs practices — and found general practice makes a 7.6% annual loss — as revealed in The Prescription for Privatisation on this platform.
Independent analysis shows practices need $353 million to $1.36 billion to address unmet need. This government offered 4–5%. The General Practice Leaders' Forum rejected it.
The Waitangi Tribunal's WAI 2575 inquiry found the Crown breached Te Tiriti o Waitangi by
"failing to design and administer the current primary health care system to actively address persistent Māori health inequities,"
as documented in The Prescription for Privatisation.
The Tribunal calculated $531 million in cumulative losses to Māori health providers between 2003–2018 — and estimated the annual health loss at $5 billion in 2018 alone. This government is not confused about the consequences. They are choosing them.
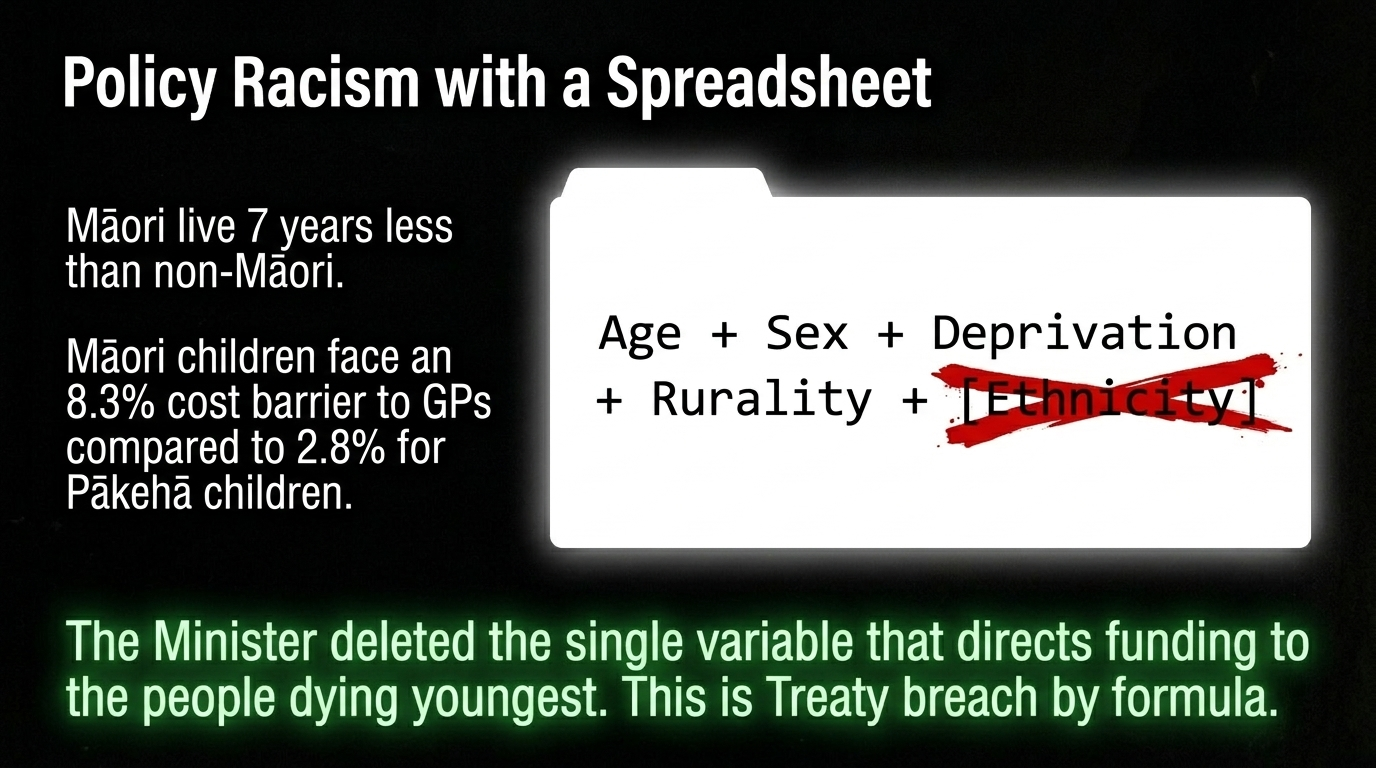
The Ethnicity Erasure: Simeon Brown Hid Racism Inside a Formula
The government's "new" capitation reweighting — scheduled for July 2026 — was supposed to modernise a 20-year-old formula.
The 2022 Sapere report, publicly funded and thoroughly evidenced, recommended including age, sex, ethnicity, deprivation, morbidity, and rurality.
Simeon Brown took the formula, deleted ethnicity, and called it an improvement.
As Dr Gabrielle McDonald of Otago University told Te Ao Māori News:
"It's illogical. Leaving ethnicity out means [funding is] not going to be allocated to those highest areas of need, which will make accessing health care more difficult for Māori and Pacific communities."
Māori live seven years less than non-Māori. Māori children bear higher death rates in almost every category. The minister deleted the one variable that would have directed money toward the people dying youngest.
Dr McDonald said this reflected a
"wider trend in government policy"
— a deliberate pushback against acknowledging ethnic need even where the evidence demands it. This is not oversight. It is policy racism with a spreadsheet. It is Treaty breach by formula.
The Privatisation Architecture: Name the Players, Follow the Money
This is where this essay goes further than any RNZ report or NZ Herald opinion piece. The GP crisis is not the whole story. It is the visible surface of a systematic privatisation of the entire New Zealand health system — and the architects have names.
Christopher Luxon — The CEO Who Came to Sell
Christopher Luxon is not a health administrator. He is a corporate executive who ran Air New Zealand — a company that, under his leadership, operated on the premise that everything that can be outsourced should be outsourced. He brought that ideology to the Beehive.
As reported by Wikipedia's entry on the Sixth National Government, the coalition's agenda from day one embedded privatisation through
"restructuring," "efficiency," and "partnership with the private sector"
— language so mundane that most people did not notice the theft occurring beneath it.
Under his watch, National raised an unprecedented $2.3 million war chest from richlist donors before his first election — money from the same private health sector now receiving public contracts. The conflict of interest is structural and undeniable.
Simeon Brown — The Health Minister Who Serves Shareholders
Simeon Brown is the most dangerous health minister in living memory
— not because he is incompetent, but because he is competent at doing exactly what his backers want. In March 2025, as confirmed by Stuff's reporting, Brown directed Health NZ Commissioner Lester Levy to offer private hospitals 10-year contracts
— locking public procurement into a concentrated corporate market before any competitive assessment had been done.
Brown ordered Health NZ to outsource 10,579 procedures by June 2025, diverting $50 million to private companies, as reported by World Socialist Web Site.
By 2026, outsourcing costs had nearly doubled to $317 million while volumes rose by only a third, as B2B News revealed. Health NZ's own executives told Brown in January 2025 that outsourcing to private hospitals was more expensive than expanding public capacity.
The strategy proceeded anyway. Brown blanked out 12 of 13 risk mitigation strategies before releasing the relevant policy memo to the public.
Available evidence suggests Brown has held private meetings with Southern Cross Health Insurance
— an aide-mémoire proactively released by the Ministry of Health confirms a 1 July 2025 meeting between the minister and Southern Cross
— while simultaneously directing public funds toward Southern Cross's hospital network.
The public interest question this raises is unambiguous: who is this minister working for?
Professor Lester Levy — The Commissioner Who "Cooked the Books"
When the government needed someone to manage the optics of gutting Health NZ, they reached for Professor Lester Levy — an Auckland University of Technology business professor and board director whose specialty is financial turnarounds, not health systems.
As Wikipedia's entry on Levy confirms, he was appointed board chair in May 2024, then the board was sacked and he became commissioner in July 2024
— accumulating unprecedented power over the country's entire health bureaucracy while simultaneously teaching two days a week at AUT.
Under Levy's tenure, Health NZ was accused of
"cooking the books"
— revising its deficit for 2023/24 from nearly $1 billion to $722 million in circumstances the Auditor-General found troubling enough to require $212 million in costs to be shifted to the next year's accounts, as Newstalk ZB reported.
Former CFO Rosalie Hughes, who resigned during a restructure, blew the whistle on Levy's accounting approach to the Auditor-General. Meanwhile, 2,000+ jobs were cut, the Director-General of Health Dr Diana Sarfati resigned, and
— as the PSA stated publicly
— the Health Infrastructure Plan under Levy and Brown began "ushering in privatisation of the health system" through public-private partnerships for hospital buildings.
This is the man they installed to "fix" Health NZ. He did not fix it. He prepared it for sale.
The Three Corporate Beneficiaries

Three companies now control 70% of the private hospital market and are the direct beneficiaries of this government's deliberate dismantling of public capacity, as B2B News reports:
Southern Cross Healthcare
— New Zealand's largest private health network, operating 11 hospitals, covering 810,000 New Zealanders with insurance, announcing a major redevelopment of its North Harbour Hospital to expand from 8 to 15 operating theatres, as Southern Cross confirmed in December 2025. Southern Cross's cost of claims rose 15%
— compared to only 9% growth in premiums
— meaning the company is under financial pressure that government contracts conveniently relieve.
Evolution Healthcare
— A for-profit private hospital operator running six hospitals, four day surgeries, and a maternity hospital, that has explicitly told the NZ Herald it is "continuing to increase its footprint, as it works more closely with government." Evolution is co-owner (with Southern Cross) of Tauranga's Grace Hospital
— the only private general hospital in the Bay of Plenty, directly relevant to whānau in our region. Evolution has been simultaneously seeking Commerce Commission clearance to acquire further surgical facilities, further concentrating market power in Wellington, as Commerce Commission documents reveal.
Healthcare Holdings / MercyAscot
— Associated with Warehouse founder Stephen Tindall, this third major player completes a market oligopoly that faces no meaningful competitive discipline
— particularly once 10-year government contracts are locked in, as B2B News confirms. Locking a dominant buyer
— the Crown — into decade-long arrangements with three dominant sellers "surrenders negotiating leverage before establishing what fair pricing looks like."
The conclusion is unavoidable: this government has manufactured a public health crisis, used it to justify privatisation, and is now locking in those private arrangements before it loses the election. The 2026 election is not a deadline. It is a fire sale.
Three Examples for the Western Mind
Example 1: The Māori Child Who Cannot See a Doctor
The harm: Māori children aged 12–24 months face cost barriers to seeing a GP at 8.3% — compared to 2.8% for New Zealand European children. Māori adults face 22% cost barriers compared to 13% for non-Māori. Māori face prescription cost barriers at three times the non-Māori rate — 14% versus 5% — as documented in The Prescription for Privatisation. After adjusting for income and deprivation, Māori still face a 37% excess in inability to see a GP, as peer-reviewed research in Family Practice confirms.
Tikanga impact — for the western mind: In te ao Māori, hauora (wellbeing) is not individual — it is collective and relational. The wellbeing of the tamaiti is inseparable from the wellbeing of the whānau, hapū, iwi. When a child cannot access healthcare, it ruptures the entire web of relationships that define a people. The Pākehā health system treats this as a statistic. Te ao Māori understands it as an attack on whakapapa — the living chain of ancestors and descendants that makes a people who they are. You would not accept a system that denied your child a doctor. We will not accept it either.
Solution: Immediate fee-free GP access for all Māori and Pacific tamariki — funded as a non-negotiable Te Tiriti constitutional obligation.
Example 2: The Rural Māori GP Desert — Right Here in the Bay of Plenty
The harm: Of the $907 million in capitation funding in 2017/18, only $28.7 million (3.1%) went to Māori health services, as revealed by The Prescription for Privatisation. Without ethnicity in the new capitation formula, rural funding flows to rural Pākehā communities, not rural Māori ones, as Dr McDonald's analysis confirms. Meanwhile, Evolution Healthcare and Southern Cross have invested in and expanded Grace Hospital in Tauranga — the Bay of Plenty's only private general hospital — while Bay of Plenty's public health services are being hollowed out. Rural Māori communities from Te Puke to Ōpōtiki face GP deserts. The corporate hospital in Tauranga serves those who can pay. The formula is designed to keep it that way.
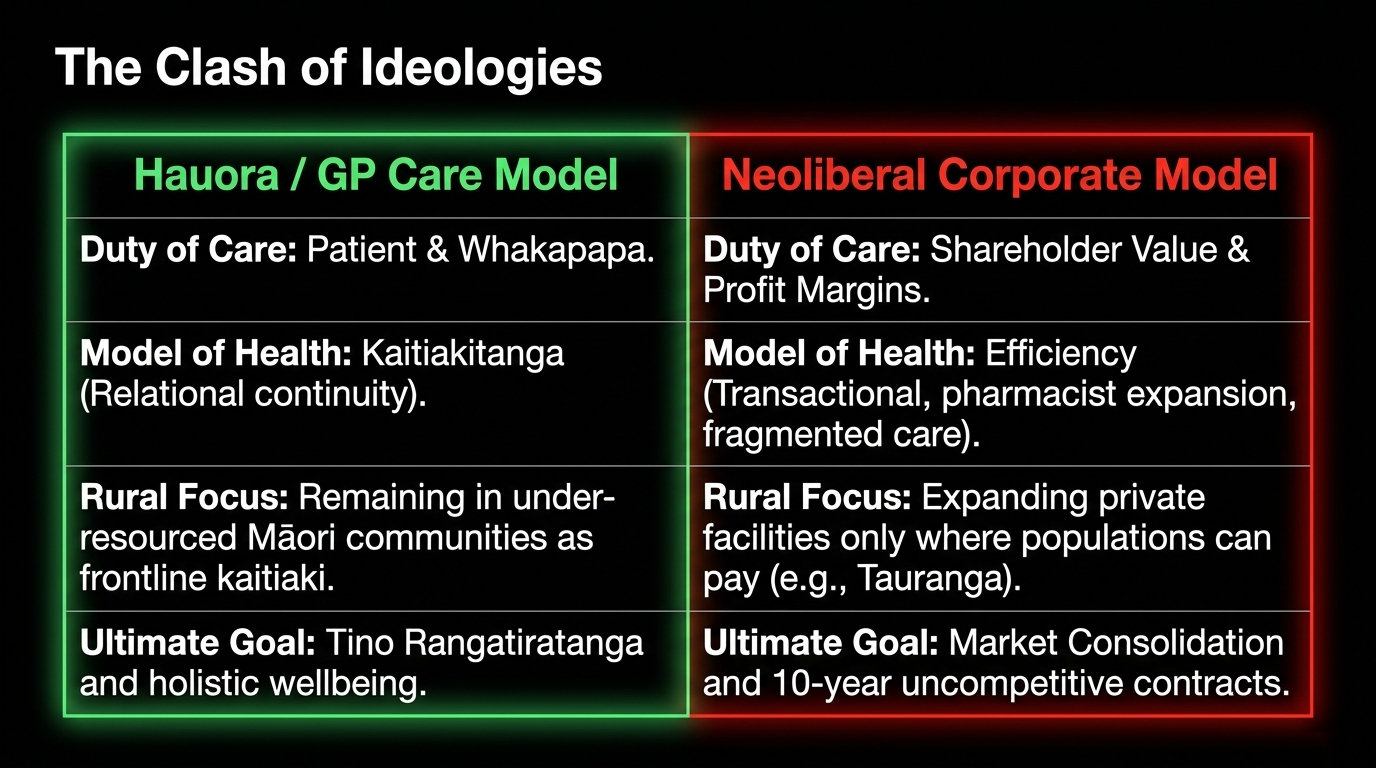
Tikanga impact — for the western mind: Kaitiakitanga is guardianship. GPs who stay in under-resourced Māori communities are kaitiaki of their people's health. When they leave — because the government has made it economically impossible to stay — the community loses not just a service but its capacity for self-determination in health. The Pākehā framework calls this a "market failure." The Māori framework calls it the destruction of a taonga.
Solution: Targeted, bonded GP placements for Māori and Pacific communities — ethnicity-weighted, properly resourced, and located in the communities that need them most.
Example 3: The Corporate Vulture and the 10-Year Contract
The harm: Every GP who closes their books is a door swung open to corporate consolidation. As previously exposed in The Corporate Vultures Circle as Our Health System Burns and The Pharmacy Con: Simeon Brown's Privatisation by Stealth, the Luxon government is deliberately starving public primary care to justify corporate takeover. Brown directed Health NZ to issue 10-year outsourcing contracts to private hospitals — locking the Crown into monopolistic arrangements with three companies that control 70% of the market — as B2B News documents. Outsourcing costs nearly doubled to $317 million in a single year. The pricing of every contract was hidden from taxpayers. The PSA warned this is the thin end of the wedge. Dr Graham Roper explicitly stated that "Māori and Pacific people and people in rural areas were unlikely to benefit from the increased use of the private sector."
Tikanga impact — for the western mind: Manaakitanga — the ethic of genuine care and reciprocal obligation — is annihilated by the corporate model. A corporate clinic's duty is to shareholders. A GP's duty is to the patient. When the system forces GPs out and corporates in, what is lost is the relational, whakapapa-grounded model of care that Māori wellbeing requires. The Pākehā calls it "efficiency." We call it the theft of healing.
Solution: Legislative prohibition on corporate buyout of GP practices in communities with high Māori and Pacific enrolment rates. Restoration of Te Aka Whai Ora. Full transparency and public disclosure of every private health contract.
The "Anti-GP Ideology" — Name the Architecture
Dr Cunningham's phrase — "anti-GP ideology" — points to something deliberate. The Ministry of Health has systematically pushed care away from GPs toward nurse practitioners, pharmacists, and urgent care centres.
This is not innovation.
It is the dismantling of continuity of care — the one factor that keeps Māori whānau alive through chronic illness.
As exposed in The Pharmacy Con: Simeon Brown's Privatisation by Stealth, Brown's pharmacist expansion fits precisely this pattern: deskill the GP, fragment the care, open the door to market actors who do not know the patient's name, whakapapa, or history.
This government dismantled Te Aka Whai Ora in February 2024, disestablishing 125 hauora Māori workers and returning responsibility to Health NZ — a bureaucracy the Waitangi Tribunal had already found was complicit in Māori health inequity.
The PSA confirmed that Dr Diana Sarfati's resignation as Director-General of Health was
"a further symptom of the Government's chaotic mismanagement and underfunding of the health system."
Peer-reviewed research in PubMed confirms:
"For more than a century, Māori have experienced poorer health than non-Māori. In 2019 an independent Tribunal found the Government had breached Te Tiriti o Waitangi by failing to design and administer the current primary health care system to actively address persistent Māori health inequities."
The Luxon government's response was to make it worse — and call it progress.
As Te Pāti Māori MP Mariameno Kapa-Kingi stated, this is a government with a "mission to exterminate Māori." On primary care alone, the evidence makes that charge impossible to dismiss.
The MGL Archive: We Have Been Naming This — Essay by Essay
The architecture of this crisis has been documented on this platform. The 1000 essays that led to this moment include:
- A House on Fire: Neoliberalism's Assault on Public Healthcare in Aotearoa — January 2025
- The Pharmacy Con: Simeon Brown's Privatisation by Stealth — exposing the pharmacist expansion agenda
- The Prescription for Privatisation — October 2025, tracing the Waitangi Tribunal's $531 million finding and the Sapere report the government buried
- The Manufactured Crisis: How They Gut Public Healthcare to Justify Privatisation — June 2025
- The Corporate Vultures Circle as Our Health System Burns — September 2025
- The Budget Band-Aid: How Government Spin Masks a Systemic Crisis — May 2025
- KO TE WHARE HAUORA KUA HEREA: The Man Who Sold the Healing House From the Inside — April 2026
- Neoliberal Vultures Circle as Health NZ Bleeds — exposing Lester Levy
- Health NZ: A Billion-Dollar Black Hole Swallowing Public Trust Whole — tracing the $722 million deficit and its political manufacture
The pattern is consistent. The architects are the same. The victims are the same.
He Poropiti: The 2026 Election — What Will Happen on 7 November
The election is confirmed for Saturday, 7 November 2026, as Wikipedia's 2026 election article records. By that date, the 54th Parliament will be dissolved, party advertising will have run for three months, and every whānau in Aotearoa will have had the opportunity to decide what kind of country they want to live in.
Here is what the verified polling data tells us, and here is The Māori Green Lantern's assessment — stated clearly as informed political analysis, not prophecy:
The Roy Morgan Poll of March 2026 shows the National-led Government (National, ACT, NZ First) on 47.5% — effectively tied with the Labour-Greens-Te Pāti Māori opposition on 48%.
The seat projection: 60 seats each. A hung Parliament. By February 2026, National had already sunk to its lowest result under Luxon in Taxpayers' Union-Curia polling. Former PM Sir John Key publicly offered advice — never a good sign for a sitting prime minister. NZ First has surged to its best result ever — but its voters are volatile and its presence in coalition makes every policy negotiation a hostage situation. A Newstalk ZB poll from August 2025 already showed Labour at 33.6%, ahead of National at 31.8%, with Greens at 9.8%.
Te Pāti Māori holds six of the seven Māori seats — and as The Spinoff reports, Labour, Greens, and Te Pāti Māori are now coordinating seriously ahead of the election. Two polls by early 2026 showed the Labour/Greens/Te Pāti Māori bloc with enough support to form government.
The Māori Green Lantern's assessment: This election will be decided on the Māori seats. If Te Pāti Māori holds all six, the left bloc wins. If the Greens pick up a Māori seat — as their new candidates suggest they will contest — the left bloc wins comfortably.
The key variable is Māori voter turnout.
When Māori whānau vote in high numbers, the right loses. That is not coincidence. That is why this government has spent three years suppressing Māori political power — killing the Māori Health Authority, attacking He Puapua, stripping Treaty references from legislation. A Māori who is sick, poor, and without a GP is less likely to vote.
The prediction: The left bloc — Labour, Greens, Te Pāti Māori — wins the 7 November 2026 election. Not by a landslide. By the determination of whānau who have had enough. The privatisation fire sale stops. The reckoning begins.
But only if we organise now. Only if whānau are informed. Only if this platform reaches 50,000 readers by November.
That is the work. That is essay 1000. That is why this voice must continue.
He Ara Whakamua — The Path Forward
For every $1 invested in primary care, $14 is saved in hospital costs, as the RNZCGP has documented.
Underfunding GPs is not fiscal prudence. It is a political choice with a body count.
The path forward requires:
- Immediate substantial funding increases — the Sapere-recommended 34–231% for high-needs practices, not the contemptuous 4–5% on offer
- Reinstate ethnicity into the capitation formula — as the Sapere report required and Dr McDonald demands
- Restore Te Aka Whai Ora with real funding, real power, real tino rangatiratanga — not a Ministry-controlled imitation
- Fee-free GP access for all Māori and Pacific whānau as a non-negotiable Te Tiriti obligation
- Dedicated Māori and Pacific GP workforce pipeline — targeted, bonded, properly resourced
- Cancel the 10-year private hospital contracts and restore public procurement transparency
- Prohibit corporate consolidation of GP practices in high-needs communities
- Pay the $531 million debt owed to Māori health providers under Waitangi Tribunal findings
- Elect a government that treats healthcare as a public good, not a corporate opportunity
This is what rangatiratanga looks like in primary healthcare. Not a funding tweak. A reckoning.
Koha — Ka Ora Te Kōrero, Ka Ora Ai Te Whānau

One thousand essays. One thousand acts of refusing to let the lie stand. Each one funded not by corporate advertisers, government grants, or mainstream media goodwill — but by whānau who decided that truth deserves a fighting fund.
When Māori cannot afford to see their GP — when the waiting room becomes a grave because the minister deleted "ethnicity" from a formula, because a commissioner "cooked the books," because three companies now hold 10-year contracts over our bodies
— the least this platform can do is make sure whānau know exactly who made that choice, and exactly what it cost.
Every koha to The Māori Green Lantern is an act of rangatiratanga.
It signals that we will fund our own truth tellers — because the Crown, the corporates, and the media they advertise in never will.
This is essay 1000.
Help us get to 2000. Help us reach 50,000 whānau before 7 November.
If you are able, koha here:
- 💰 Koha platform: Support The Māori Green Lantern
- 📖 Subscribe — essays direct to your kete: themaorigreenlantern.maori.nz
- 🏦 Direct bank transfer: HTDM — 03-1546-0415173-000
- 👍 Follow and share on Facebook: The Māori Green Lantern
If you cannot koha — no worries. Subscribe, follow, kōrero, share with your whānau and friends.
That is koha in itself.
Every share puts this analysis in front of someone who needs it before 7 November. That is how we build the media the Crown will never fund for us.
Kia kaha, whānau. Stay vigilant. Stay connected. The waiting room is not a grave — not while we still have a voice.
Views expressed constitute honest opinion on matters of public interest under the Defamation Act 1992 (NZ) and Durie v Gardiner * NZCA 278. All factual claims sourced and cited. Named individuals — Christopher Luxon, Simeon Brown, and Lester Levy — referenced solely in their public capacity as elected officials and public appointees. Predictions regarding election outcomes are stated as informed political analysis, not fact. Errors and corrections: themaorigreenlantern.maori.nz*